
Research
Exercise
April 10, 2025
How Postpartum Exercise Affects Diastasis Recti and Pelvic Floor Dysfunction

Introduction
Pelvic floor dysfunction and diastasis recti abdominis (DRA) are common after childbirth, often affecting a woman’s quality of life long after delivery. Issues like urinary incontinence, pelvic organ prolapse, and sexual dysfunction can persist, creating a need for effective rehab strategies.
While exercise is widely recommended as a first-line treatment, its effectiveness— especially in the first year postpartum—remains understudied. This systematic review examines the latest evidence on the effects of exercise for pelvic floor dysfunctions and DRA, shaping future guidelines for postpartum care.
Method
Population
This review focused on individuals within their first year postpartum. Studies with participants beyond 12 months were only included if the intervention started before the one-year mark.
Intervention (exposure).
This review examined the effects of any form of postpartum exercise on pelvic floor dysfunctions, whether measured objectively (e.g., trackers) or subjectively (e.g., self- reported). It included:
- All types (strength, aerobic, pelvic floor, etc.), intensities, and durations—from single sessions to long-term programs.
- Exercise programs (e.g., pelvic floor training) and combined interventions (e.g., exercise + biofeedback), though exercise-only groups were analyzed when both were present.
- Interventions starting in the first year postpartum, even if they began during pregnancy (as long as most occurred after delivery). When available, extended follow-up data was categorized into two phases: the maintenance phase (post- intervention to follow-up) evaluated sustained effects, while the long-term effect analysis (baseline to follow-up) provided insight into cumulative benefits.
The review included studies comparing postpartum effects of exercise for pelvic floor dysfunctions against various control conditions: no intervention (including standard care), minimal contact approaches (such as online programs or education-only), alternative exercise protocols (varying in frequency, intensity, duration, volume or type), and active control groups (like low-intensity exercise programs).
This broad range of comparators allowed for comprehensive evaluation of the effectiveness of exercise on pelvic floor dysfunctions across different implementation approaches.
Outcomes and Assessment Methods
The study evaluated five key outcomes – urinary incontinence, anal incontinence, pelvic organ prolapses, sexual function, and diastasis recti abdominis (DRA) – using both subjective measures (including validated tools like the Urinary Distress Inventory and ICIQ-UI Short Form for symptom reporting) and objective clinical assessments (particularly calipers or ultrasound imaging for quantifying inter-rectus distance in DRA cases).
Study design
The review included all primary study designs except single-case reports, narrative syntheses, and systematic reviews.
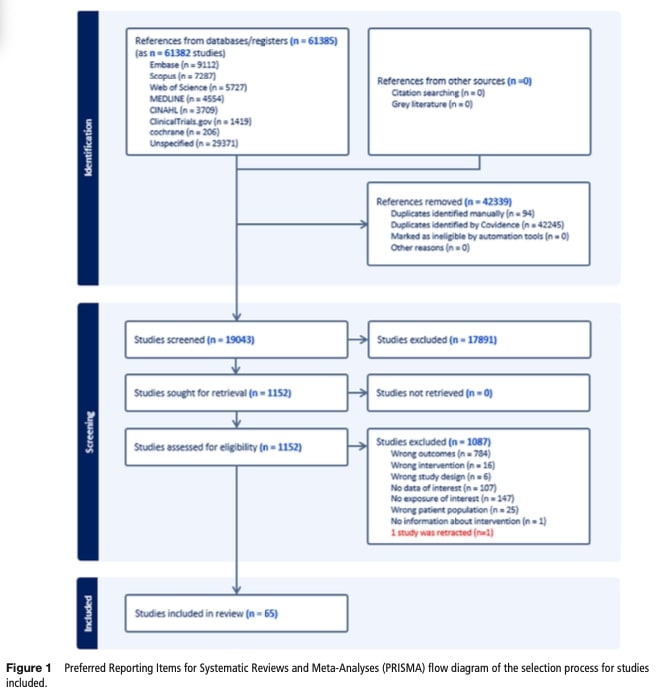
Study selection and data extraction
Search results were deduplicated in Covidence, then screened independently by two reviewers. Articles meeting criteria underwent full-text review, with disagreements resolved by consensus. Two reviewers extracted data using standardized forms, verified by an expert, covering study design, interventions, and outcomes, supplementing with author queries when needed.
Certainty of Evidence Assessment
The evidence certainty was evaluated using the GRADE framework. Randomized controlled trials (RCTs) started as high-certainty evidence but were downgraded for risk of bias, indirectness, inconsistency, imprecision, or publication bias. Non-RCTs and observational studies began as low-certainty evidence but could be upgraded for strong effects or dose-response relationships.
Two reviewers independently assessed risk of bias using modified Joanna Briggs Institute (JBI) criteria, evaluating study design, measurement accuracy, confounding factors, and statistical methods. Disagreements were resolved through discussion.
The researchers assessed potential limitations in the evidence by examining four key factors:
Inconsistency between study results was evaluated using Cochran’s Q test and I2 statistics, with an I2 value exceeding 50% indicating substantial heterogeneity that required further investigation.
Indirectness was considered when significant variations existed in study populations or intervention protocols.
Imprecision was identified when studies had small sample sizes (fewer than 300 participants per group) or excessively wide confidence intervals.
Publication bias was only examined in meta-analyses that included at least 10 studies, as smaller numbers of studies make such assessment unreliable.
Results
Pelvic Floor Training
Most high-quality studies examined pelvic floor muscle exercises. Programs varied significantly:
- Some women did short 5-minute sessions, others exercised up to 3 times daily
- Programs started anywhere from late pregnancy to 6 months after birth
- Most used targeted pelvic floor exercises alone, while a few added special toolslike biofeedback
- Surprisingly, no studies tested regular fitness programs (like cardio or strength training)
Abdominal Recovery
For abdominal separation (diastasis recti), 28 studies showed:
- Best results came from specific abdominal exercises, sometimes combined withpelvic floor work
- Some programs used extra support like special tapes or binders
- Exercise timing varied greatly – some started right after birth, others began up toa year later
Sessions lasted 5-50 minutes, done anywhere from weekly to daily
The certainty of evidence across studies varied from high to very low. The most frequent limitation was imprecision, primarily due to small sample sizes that reduced statistical power to detect meaningful effects. Many studies were also downgraded for indirectness, as they often combined exercise with co-interventions (e.g., biofeedback, electrical stimulation, or posture training), making it difficult to isolate the specific impact of exercise on pelvic floor dysfunctions. Publication bias could not be assessed because most meta-analyses included fewer than 10 studies.
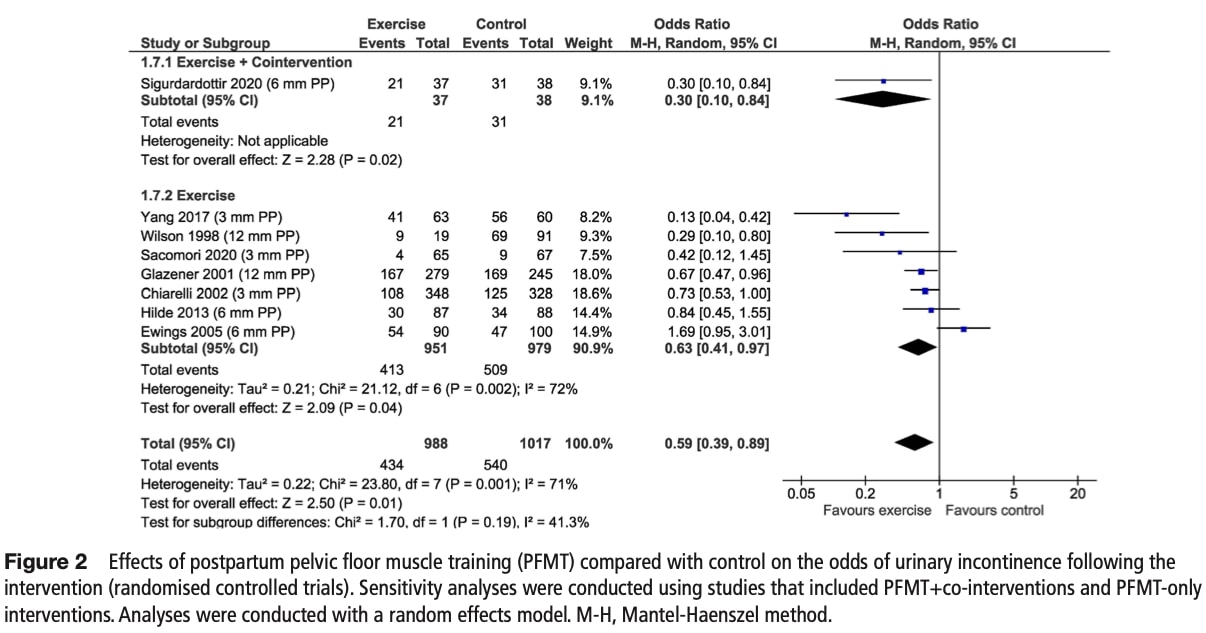
Risk of urinary incontinence:
Post-intervention analysis of eight RCTs revealed pelvic floor muscle training significantly reduced incontinence odds by 41% though with moderate heterogeneity (I2=71%). The evidence certainty was rated moderate, downgraded for indirectness due to varied co- interventions across studies.
Sensitivity Analysis: No significant difference between pelvic floor-only training (OR 0.63) and combined interventions (OR 0.30), though the latter showed a stronger (but non- significant) effect.
Subgroup Analyses: No statistically meaningful differences based on:
- Intervention timing postpartum (p=0.71)
- Delivery mode (vaginal/C-section; p=0.74)
- Supervision level or program type (both p=0.38)
- Exercise type and start timing could not be analyzed due to insufficient data.
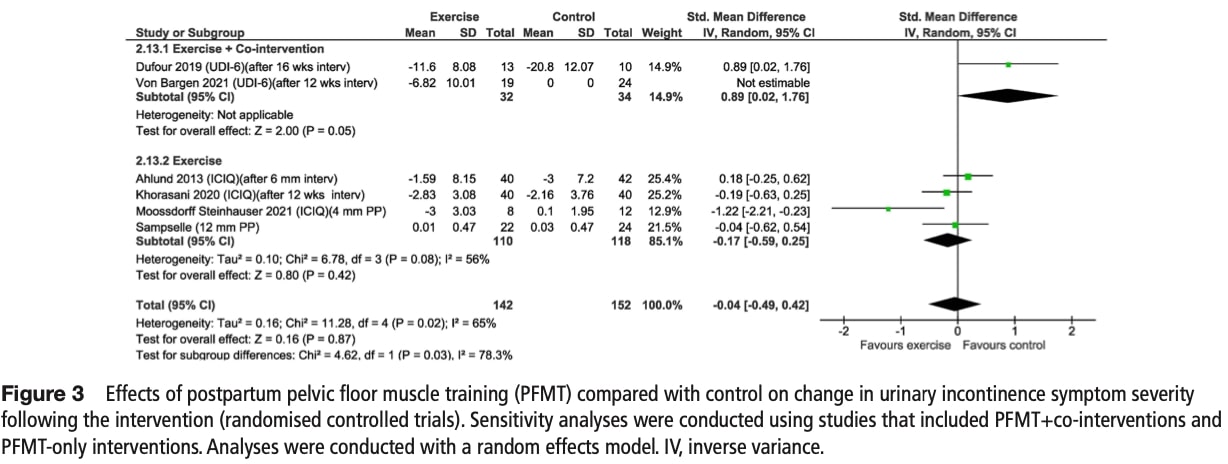
Changes in urinary incontinence symptom severity
The pooled analysis showed no significant improvement in symptom severity with pelvic floor muscle training (PFMT) versus control, with very low-certainty evidence due to heterogeneity and imprecision.
Sensitivity Analyses
- PFMT alone showed no benefit, while combined interventions (PFMT + co-
therapies) paradoxically increased symptom severity versus controls (p=0.03). Subgroup Analyses
- Supervised group training significantly reduced severity (SMD – 1.22, moderate certainty).
- Unsupervised home programs had no effect.
- No differences were seen by timing or delivery mode (all p>0.05).
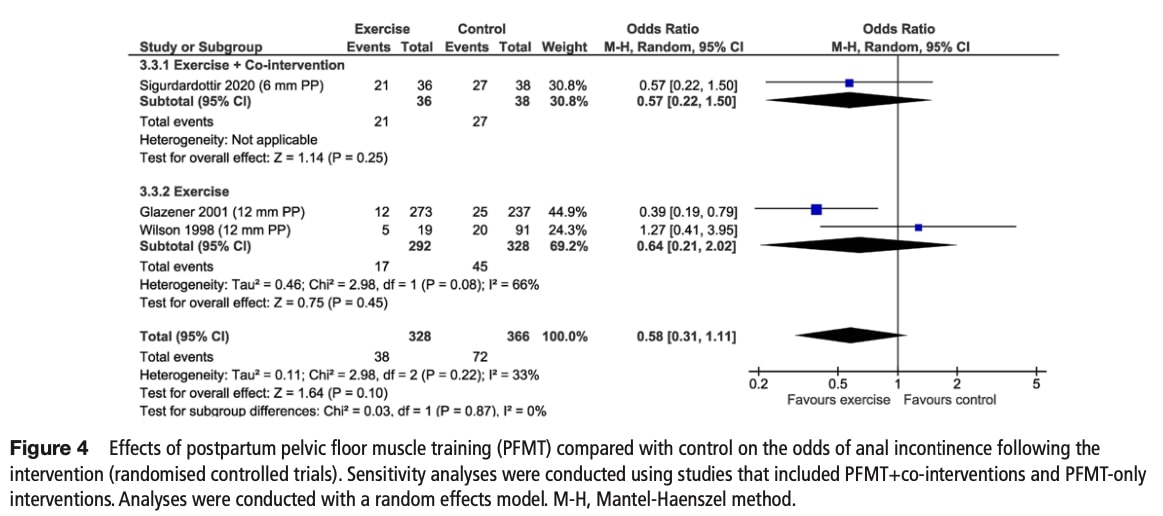
Risk of anal incontinence
Post-intervention analysis suggested a 42% reduction in odds with PFMT, though this did not reach statistical significance. Evidence certainty was low, downgraded for indirectness and imprecision.
Sensitivity Analysis:
- No difference between PFMT-only and combined interventions (p=0.87).
Subgroup Analyses:
- No significant effects based on intervention timing postpartum (p=0.08).
- Other subgroups (delivery mode, exercise type, etc.) lacked sufficient data.
Changes in anal incontinence symptom severity
One RCT found that combined pelvic floor muscle training (PFMT) and co-interventions reduced anal incontinence symptoms more than control, measured by the Colorectal- Anal Distress Inventory.
However, evidence certainty was low due to the small sample size and use of combined therapies rather than PFMT alone. While results suggest potential benefit, the narrow statistical significance (CI barely excluding zero) and study limitations mean conclusions remain tentative. Larger studies are needed to verify these findings.
Change in sexual function.
Two randomized trials (n=118) evaluated changes in sexual function using the Female Sexual Function Index (FSFI). The combined analysis showed no significant difference between pelvic floor muscle training and control groups, with very low certainty evidence due to high inconsistency (I2=91%) and imprecision.
Sensitivity Analysis revealed opposing effects:
- PFMT alone improved sexual function in one study
- Combined PFMT+co-interventions worsened outcomes in another
- This significant difference (p=0.001) suggests intervention type critically impacts results
Subgroup Analyses could not be performed due to insufficient studies examining exercise-only approaches.
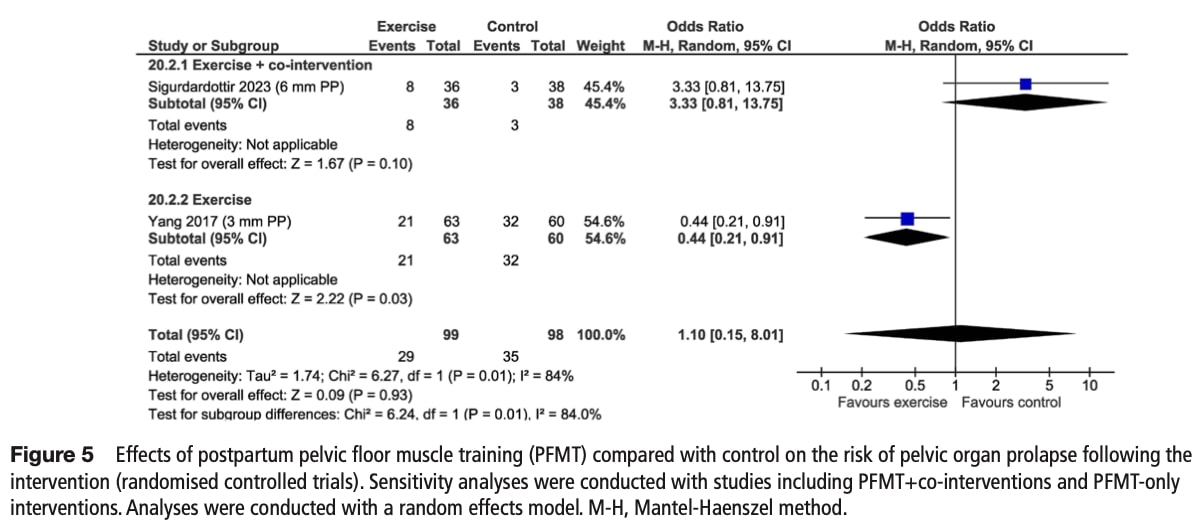
Risk of pelvic organ prolapse
Two RCTs examined whether pelvic floor muscle training (PFMT) affects pelvic organ prolapse risk. The pooled analysis found no significant difference between combined PFMT+co-interventions and controls, with low-certainty evidence due to imprecision and high heterogeneity (I2=84%).
Sensitivity Analysis:
- PFMT alone significantly reduced prolapse odds by 56%.
- Combined interventions showed no benefit.
Subgroup Analyses:
- Not feasible due to only one PFMT-only study.
This suggest that pelvic floor exercises alone may help prevent prolapse and adding other treatments might cancel out this benefit.
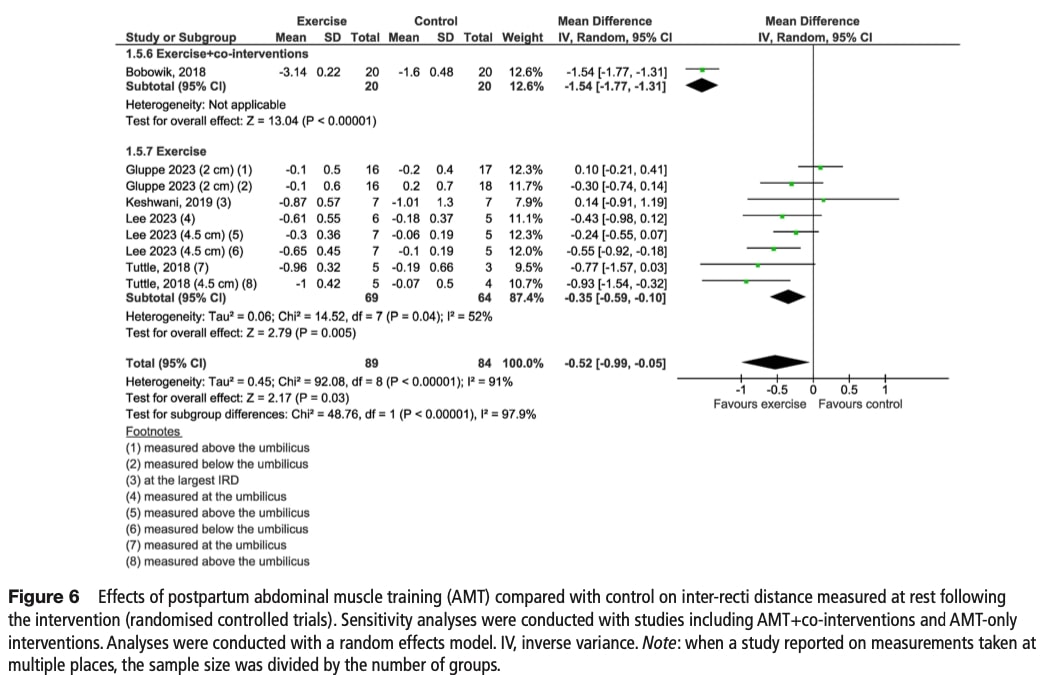
Changes in inter-recti distance measured at rest
At baseline, the average inter-rectus distance (IRD) was nearly identical between groups, aligning with general population norms (2.2 cm). Post-intervention, abdominal muscle training reduced IRD by 0.52 cm more than control, though evidence certainty was low due to indirectness (varied co-interventions) and imprecision (small samples, wide CI). Heterogeneity was very high (I2=91%).
Sensitivity Analysis:
- Combined interventions (training + co-therapies) showed greater IRD reduction (-1.54 cm) than training alone (-0.35 cm).
- Evidence certainty: Low for combined, moderate for training-only.
Subgroup Analysis:
- Unsupervised programs reduced IRD more than supervised (-0.87 cm vs. -0.35cm; p=0.02).
- No differences by measurement site, exercise type, or delivery mode (all p>0.05).
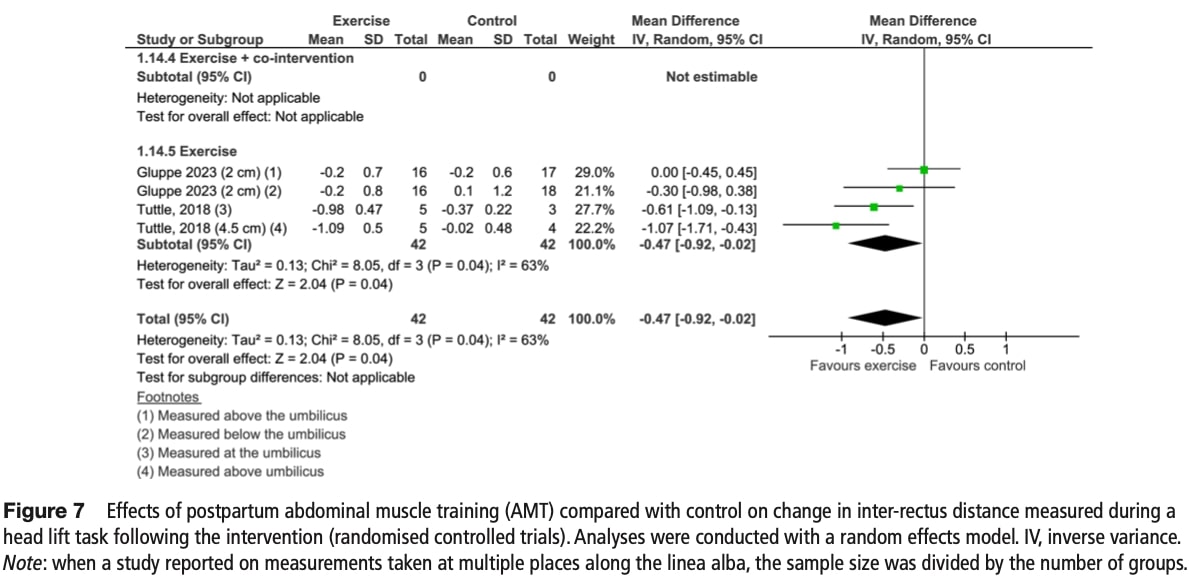
Change in inter-recti distance measured during a head lift task
At baseline, inter-rectus distance (IRD) during head lift was similar between groups. Post- intervention, abdominal training showed a 0.47 cm greater IRD reduction versus controls with moderate-certainty evidence (downgraded for imprecision). Heterogeneity was moderate (I2=63%).
Sensitivity Analysis:
- Not performed (no studies with combined interventions).
Subgroup Analysis:
- Unsupervised transverse abdominis training significantly reduced IRD (-0.79cm, moderate certainty).
- Supervised curl-up programs showed no benefit.
- No effects based on measurement site (p=0.77).
Questions and thoughts
This systematic review’s broad inclusion criteria for exercise interventions make it difficult to draw definitive conclusions about the most effective approaches for postpartum pelvic floor recovery. A major limitation is the potential dose-response relationship of pelvic floor muscle training (PFMT)—it’s possible that some studies failed to show benefits simply because the exercise dose (frequency, intensity, or duration) was too low to produce measurable effects.
Additionally, the reviewed studies included highly heterogeneous populations—some focused-on delivery-related injuries, while others examined mixed presentations like pelvic floor dysfunction with low back pain. This variability limits the generalizability of the findings, highlighting the need for better patient classification. Future research should distinguish between subgroups (e.g., women with trauma-induced pelvic floor damage vs. those with functional weakness) to determine who benefits most from PFMT versus other therapies.
The definition of a clinically meaningful cutoff for diastasis recti abdominis (DRA) remains debated. While some studies suggest a threshold of >2.2 cm, more recent research using CT scans indicates that an inter-rectus distance (IRD) of up to 3.4 cm (measured 3 cm above the umbilicus) may still fall within normal limits.
In this study, participants were included only if they presented with an IRD greater than 3.4 cm, reflecting a stricter diagnostic criterion. However, further research is needed to evaluate the effectiveness of exercise interventions for women with more severe separation (>5 cm), as current evidence in this subgroup remains limited.
Talk nerdy to me
Statistical analysis and narrative synthesis
The meta-analysis used mean differences (MD) for outcomes measured consistently (e.g., pelvic floor muscle strength in mm Hg) and standardized mean differences (SMD) when studies employed different scales (e.g., varied symptom questionnaires). SMDs, calculated via Hedges’ g, quantified effect sizes (0.2=small, 0.5=moderate, 0.8=large). For binary outcomes like incontinence prevalence, odds ratios (ORs) compared intervention vs. control groups, with OR<1 favoring exercise.
Study Grouping and Comparisons
The researchers organized the studies by their design, keeping randomized trials separate from non-randomized ones. For studies comparing different exercise programs (without a no-exercise group), they labeled the more intensive or specialized programs as “Intervention 1” and the less intensive ones as “Intervention 2.” This helped them see which approaches worked better.
Analyzing the Effects
They first checked if exercise-only programs gave different results than programs combining exercise with other treatments (like biofeedback). Then, they looked at specific factors that might influence outcomes, such as when the exercise started after birth (before or after 12 weeks), how the baby was delivered (vaginal birth or C-section), the type of exercise, and where belly muscle separation was measured.
Handling Variations in Results
Since studies often showed different results, the researchers calculated how much of this variation was meaningful (using I2 statistics). When studies differed significantly (I2 >50%), they investigated possible reasons, like differences in exercise programs or participant groups. If they found important differences (p < 0.05), they explored them further to understand what was driving the variation.
Special Approach for Belly Muscle Measurements
For studies measuring belly muscle separation, they used a special statistical method to account for multiple measurements taken from the same participants. This method separated differences into three types: measurement errors, differences within the same study, and differences between different studies. This ensured their conclusions were more accurate.
Data Inclusion and Reporting
Studies with missing or unclear data were excluded from the numerical analyses. For studies reporting results in different formats (like medians instead of averages), the researchers converted the numbers to make them comparable. When studies couldn’t be analyzed numerically, they summarized the findings in words, organizing them by study design and outcome.
Take home message
Research shows that targeted exercises for pelvic floor dysfunctions is highly effective, with these evidence-based benefits:
- 41% Lower Risk of Urinary Incontinence – Pelvic floor muscle training (PFMT) proves highly effective in preventing incontinence.
- Best Results with Supervised Group Training – Structured, professionally guided sessions deliver superior outcomes compared to home exercises alone.
- Simplicity Wins – Basic PFMT often works better than complex approaches using biofeedback or electrical stimulation.
For Diastasis Recti
- Target transverse abdominis muscles. These literature reviews may provideuseful ideas for exercises to prescribe during and after pregnancy https://app.physiotutors.com/research- reviews/abdominal-strengthening-postpartum
- Unsupervised programs frequently show better results than supervised, this could be linked to patient treatment adherence.
- Progress from basic activation training to functional movements
Clinical Recommendations
- Start Early: Begin PFMT by 2-3 months postpartum
- Explore the impact of pelvic floor dysfunctions on body perception, participation and physical function.
- Progress Smart :
- Move from static holds, which foster muscle activation, to in-situation activation based on movements that may trigger the patient’s symptoms.
- Adjust based on symptom response.
- Track symptom changes objectively by using : Urinary Distress Inventory,Short Form, Questionnaire-Urinary Incontinence Short Form.
To learn more about pelvic floor dysfunctions and physiotherapy, listen to this podcast on Physiotutors :
Pelvic Floor Physio with Dr Sarah Haag
Reference
CHALLENGE: TAKE THE QUIZ THAT 75% OF PHYSIOTHERAPISTS FAIL
Answer these 10 short questions on essential knowledge each physiotherapist should know and find out if you score better


