
Research
Exercise
March 20, 2025
Early Physiotherapy Accelerates Recovery in Subacute Mild TBI

Introduction
Traditionally, the management of mild traumatic brain injury (mTBI) relies on passive rest and gradual activity resumption. While most patients recover within four weeks, up to 30% experience persistent symptoms that may require physiotherapy. Emerging research suggests that physiotherapy after traumatic brain injury could accelerate recovery, yet most evidence comes from non-randomized trials focused on young athletes.
This study aims to fill the gap by examining the impact of early physiotherapy after traumatic brain injury versus delayed physiotherapy on balance control in a broader population, including community-dwelling adults often overlooked in mTBI care.
By integrating both self-reported symptoms and objective measures like the Central Sensorimotor Integration (CSMI) Test, researchers to explore if early physiotherapy could be the key to unlocking faster symptom resolution and enhanced motor performance.
Methods
Study Design:
This randomized controlled trial (RCT) investigated the timing of physiotherapy after traumatic brain injury (mTBI) influences recovery. Participants were randomized into two groups. The early physiotherapy group started within a week of baseline testing and the late physiotherapy group began after a 6-week waiting period. All participants underwent assessments before and after the intervention, with the late therapy group having an additional assessment before starting therapy.
Participants:
Participants were sourced from clinics in Portland, Oregon, and had to meet the following criteria: a physician-confirmed mTBI diagnosis within 2 to 12 weeks, an age range of 18 to 60 years, and moderate symptoms with a SCAT5 severity score of 15 or higher (symptom severity score range : 0-132). The Sport Concussion Assessment Tool 5 (SCAT5) is a standardized tool that scores concussion symptoms, cognitive function, balance, and neurological signs to help guide recovery and return-to-play decisions. Additionally, they needed to show no significant cognitive impairment or balance-related conditions. Exclusion criteria included severe pain, neurological disorders, substance use disorder, pregnancy, or current participation in vestibular therapy.
Sample Size & Randomization:
A total of 160 participants (80 per group) were estimated to ensure sufficient statistical power, accounting for a 20% dropout rate. An adaptive randomization method was used to balance age and sex distribution. Due to the expected higher dropout rate, 60% of participants were assigned to the late physiotherapy group, leading to 121 patients in the control group and 82 in the intervention group. While the physiotherapists administering the intervention were aware of the patient groups, the study outcome assessors remained blinded.
Intervention:
The early therapy group received rehabilitation within one week of testing, while the late therapy group received only an educational brochure for six weeks before starting therapy. Both groups then underwent eight 60-minute physiotherapy sessions over six weeks, with two sessions per week for the first two weeks and weekly sessions for the remaining four weeks. The rehabilitation intervention, detailed in a separate publication, focused on four key areas: cervical spine rehabilitation, joint position sense training, strengthening and motor control exercises, cardiovascular training using the Buffalo Treadmill Protocol, and balance training (both static on variable surfaces and dynamic).
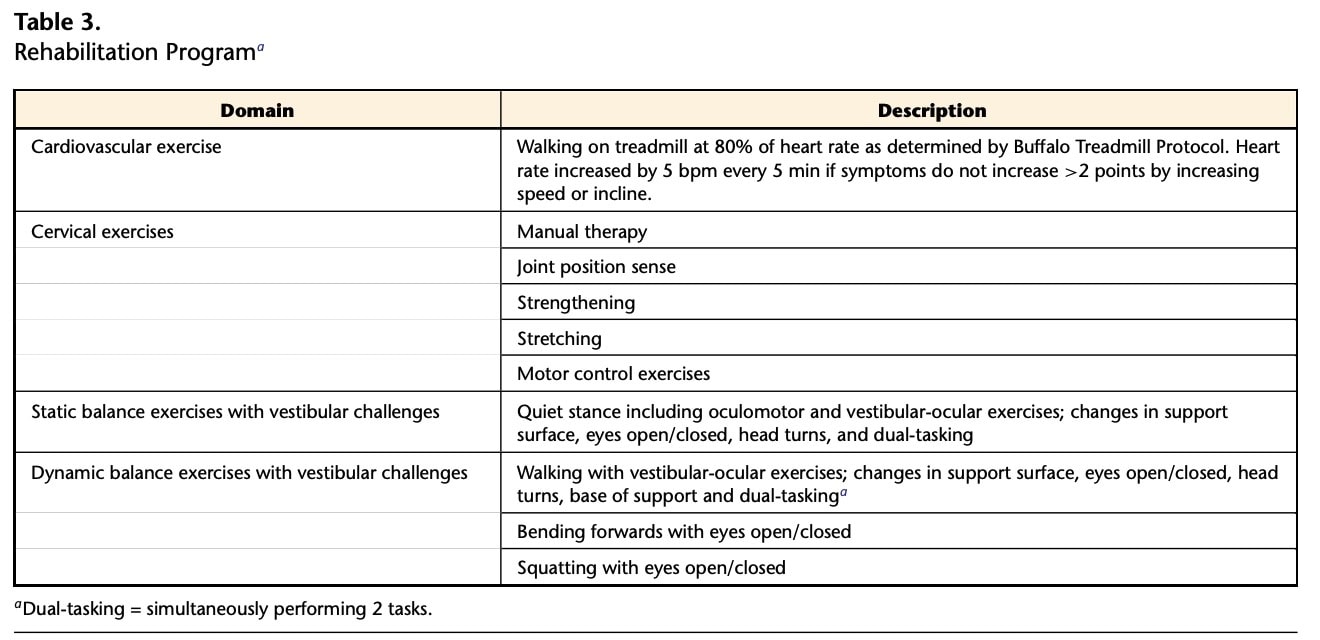
Exercises were progressively adjusted based on participant ability, and a home exercise program was included.
Outcome Measures:
Primary outcome: Dizziness Handicap Inventory (DHI), a self-administered questionnaire that measures dizziness-related disability and is reliable for test retest. Scores range from 0 to 100, with higher scores indicating a greater perceived handicap due to dizziness.
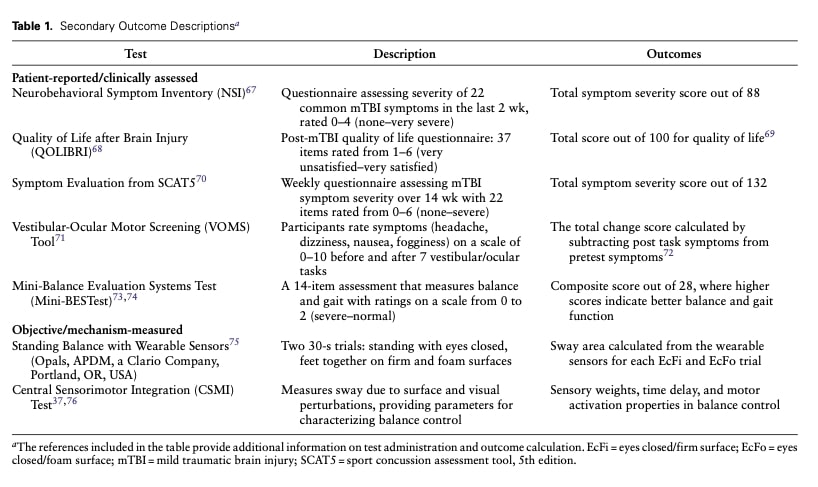
Secondary outcomes: Secondary outcomes are presented in Table 1. Symptom assessments from the Sport Concussion Assessment Tool 5th edition (SCAT5), symptom evaluation was completed weekly throughout the 14 weeks study.
The study compared demographics between the earlier and later physiotherapy groups and used a linear mixed-effects model (LME) with an intention-to-treat design to analyze outcomes. This model accounted for factors like group, time since injury, and their interaction, while also adjusting for covariates such as age, gender, and initial SCAT symptom severity. To handle dropouts, the study used inverse probability weighting, giving more weight to participants likely to drop out and less to those who completed the study, ensuring the results remained representative.
Results were reported as daily changes with 95% confidence intervals (CIs) and interaction p-values, alongside rates of change and means ± standard deviations (SDs) for a clear picture of recovery trends. To dive deeper, paired t-tests and Hedges’ G effect sizes (ESg) were used to assess changes within each group. Effect sizes were categorized as small (0.2–0.5), medium (0.5–0.8), or large (>0.8), helping to gauge the clinical significance of the findings. All analyses used a significance level of α = 0.05.
Results
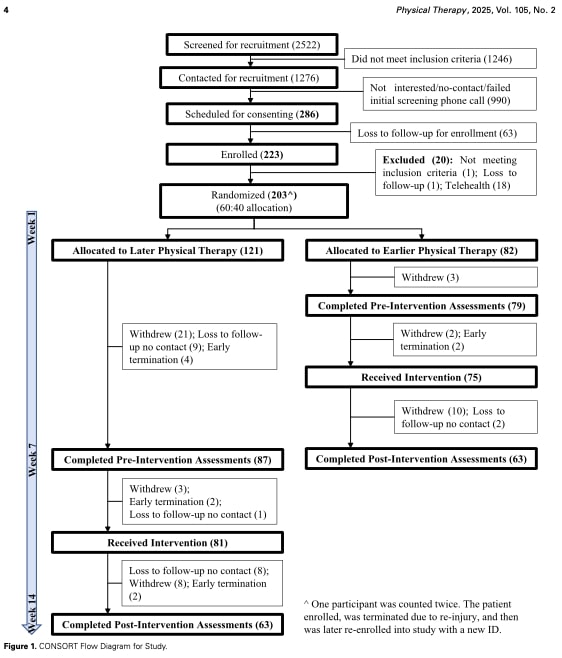
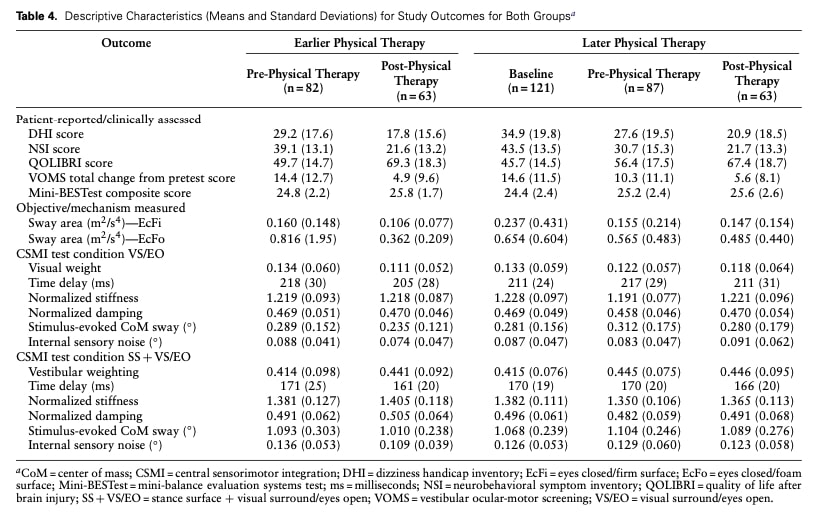
Between July 2018 and March 2023, 203 participants were randomized into an earlier physiotherapy group (n = 82) and a later physiotherapy group (n = 121). The dropout rate was higher in the later group (48%) compared to the earlier group (23%), with 63 participants from each group completing post-intervention assessments.
Primary Outcome (DHI Score):
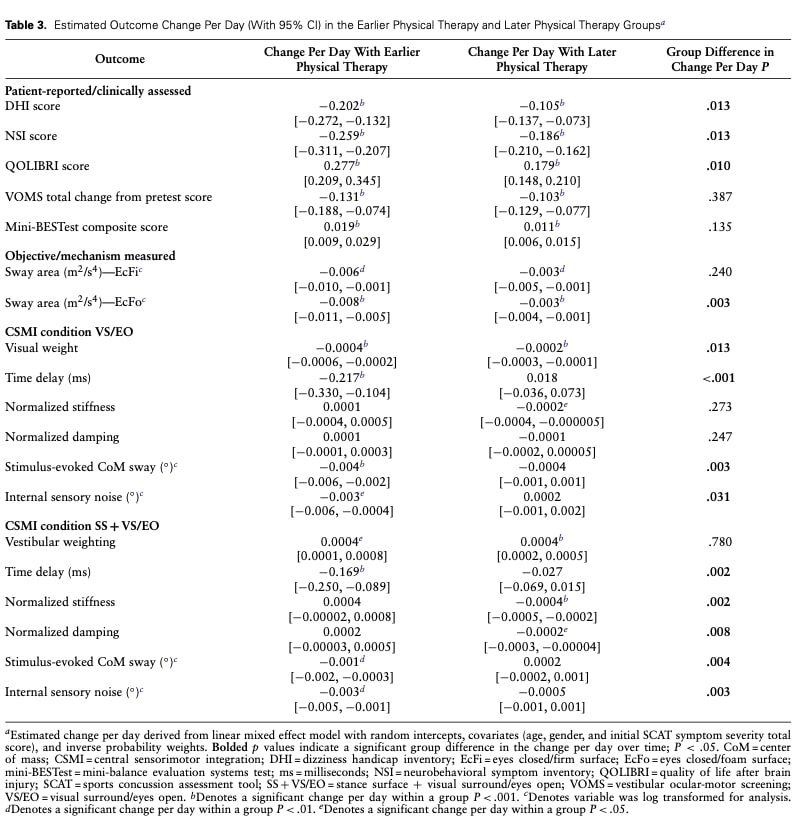
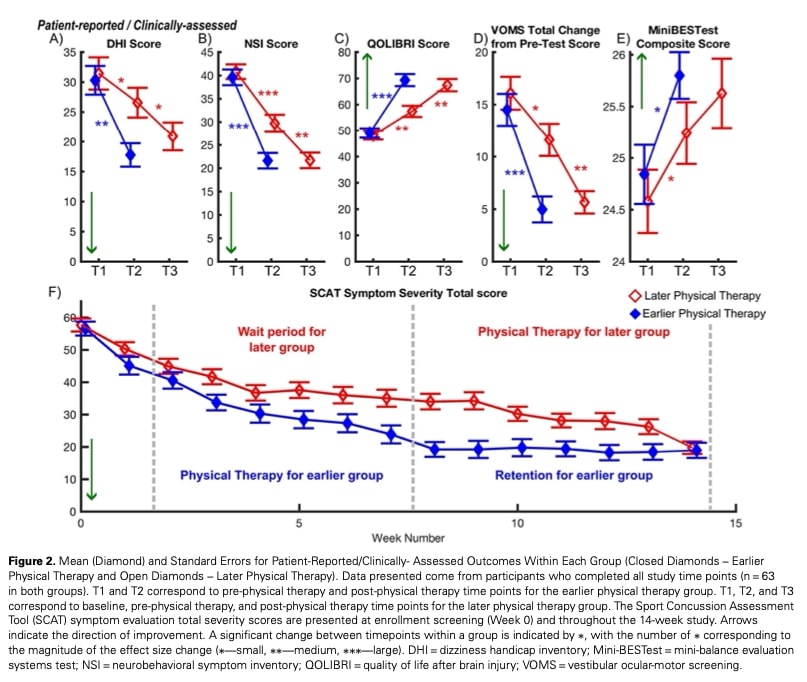
Both groups showed significant improvements, but the earlier therapy group had a larger daily reduction in Dizziness Handicap Inventory (DHI) scores compared to the later group. This means that perceived dizziness symptoms decreased faster for the earlier group, with a significant reduction in DHI scores from pre- to post-intervention. The later physiotherapy group also showed a significant reduction in DHI scores during the 6-week waiting period (from baseline to pre-therapy) and from pre- to post-therapy. However, unlike the earlier group, the effect sizes were modest, indicating that the magnitude of symptom improvement was greater in the early group.
Secondary Outcomes (Patient-Reported and Clinically-Assessed Measures):
The earlier group showed greater improvements in symptom severity (NSI) and quality of life (QOLIBRI) compared to the later group. Both groups improved in Vestibulo-Ocular Motor Screening (VOMS) and Mini-BESTest scores, but there was no significant difference in the rate of improvement between the groups. Data from the weekly SCAT5 symptom scale revealed that while both groups reached similar symptom levels by the 14-week mark, the earlier group achieved this level faster, consistent with the findings from the Dizziness Handicap Inventory (DHI).
Secondary Outcomes (Objective and Mechanistic Measures):
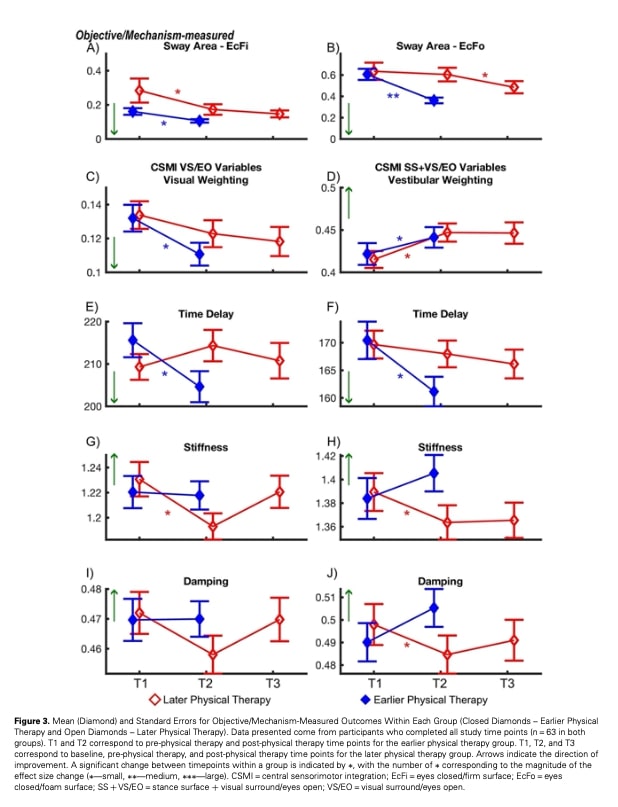
The earlier physiotherapy group showed a significantly greater daily reduction in sway area during eyes-closed foam surface (EcFo) standing balance compared to the later group. The later group showed no significant change from baseline to pre-therapy but improved post-therapy. No group differences were found for the eyes-closed firm surface sway area.
Both groups improved in visual sensory weight, meaning they relied less on visual inputs to maintain balance. The earlier group had a significantly greater daily reduction, while the later group showed no significant changes. For vestibular sensory weight, both groups improved at similar rates, with no group differences, suggesting that vestibular function may recover spontaneously after mild TBI.
The earlier group also had significantly greater daily improvements in time delay for visual surround/eyes open (VS/EO) and combined stimulus: stance surface + visual surround/eyes open (SS + VS/EO) conditions, while the later group showed no significant changes.
For motor activation parameters (stiffness and damping) in the SS + VS/EO condition, the earlier group showed no change, while the later group significantly worsened daily. This suggests that the later group has compensated by “bracing” to maintain a stable balance during this task. The later group also worsened in stiffness for the VS/EO condition from baseline to pre-therapy. Finally, the earlier group showed significantly greater daily improvements in the stimulus-evoked center of mass sway and internal sensory noise measures compared to the later group, indicating that motor control is an important focus for early physiotherapy after traumatic brain injury.
Question and thoughts
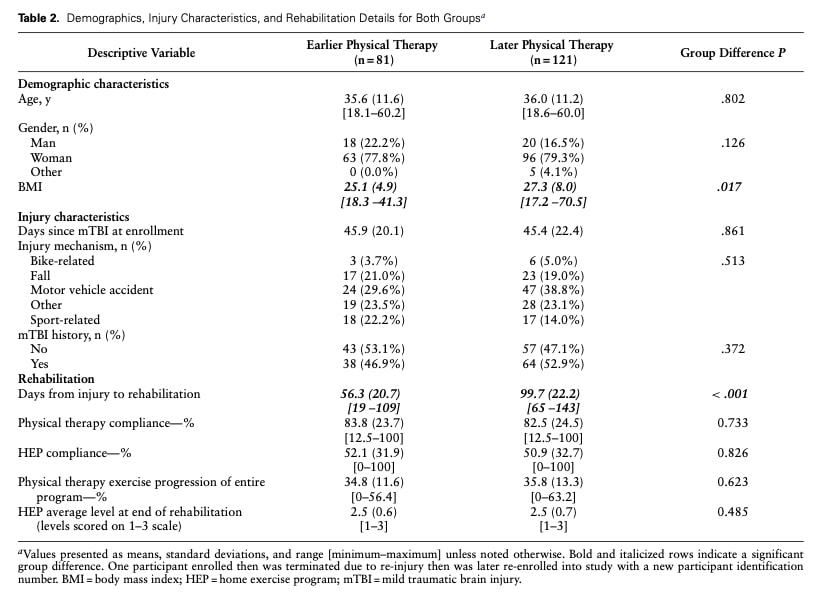
According to the data, 19 participants in the earlier group (23%) and 58 in the later group (48%) did not complete post-intervention assessments, suggesting that participants in the later group were more likely to discontinue the study. The authors reported that the primary reasons for dropout, in order of importance, were time commitment for both groups and illness for the later group. Some participants in the later group also withdrew after randomization. This low adherence might reflect patients’ perceptions of their symptoms and capabilities, leading them to underestimate their limitations and perceive the physiotherapy intervention as less necessary. To address these barriers, strategies such as shorter sessions, flexible scheduling, or enhanced patient education could improve compliance and make the intervention more feasible in real-world settings.
Additionally, the study reported a low compliance rate with the Home Exercise Program (52.1% for the earlier group and 50.9% for the later group), which could pose significant challenges in clinical practice. This low adherence may be due to the intervention protocol including too many exercises or insufficient follow-up. The improvement in Dizziness Handicap Inventory (DHI) scores for both groups, despite maladaptive motor activation patterns in the later group, suggests a potential mismatch between patients’ perceived capabilities and their actual functional limitations. This highlights the need for better patient education and closer monitoring to ensure accurate self-assessment and adherence.
Finally, while the study demonstrated the benefits of early physiotherapy after traumatic brain injury, the intervention design raises practical concerns. Each session lasted 60 minutes, which may be unrealistic in many clinical settings where follow-up sessions are typically shorter (e.g., 30 minutes). This discrepancy could limit the applicability of the study’s findings to everyday practice.
Talk nerdy to me
The study employed a combination of advanced statistical tools to analyze the effects of early versus late physiotherapy on recovery outcomes. The primary method was a linear mixed-effects model (LME) with an intention-to-treat (ITT) design. LME is particularly suited for longitudinal studies, as it handles repeated measures over time and accounts for both fixed effects (e.g., group assignment, time since injury) and random effects (e.g., individual variability). The ITT approach ensures that all participants are analyzed according to their original group assignment, even if they drop out or deviate from the protocol, thereby minimizing bias. The LME models included fixed effects for group (earlier vs. later therapy), time since injury, and their interaction, with the later group serving as the reference. Covariates such as age, gender, and initial SCAT symptom severity were incorporated to control for their potential influence on outcomes. Random intercepts were included to account for within-participant correlations. To address missing data due to dropout, inverse probability weighting (IPW) was applied. IPW assigns weights to participants based on their likelihood of completing the study, upweighting those likely to drop out and down weighting those likely to complete, ensuring the analysis remains representative of the entire study population. Sensitivity analyses were conducted to confirm the robustness of the IPW approach.
For outcomes that violated normality assumptions (meaning their data were skewed and didn’t follow a bell-shaped curve), log transformations were applied. This mathematical adjustment made the data more normally distributed, ensuring the statistical tests were valid and reliable. Results from the Linear Mixed-Effects Models (LME) were reported as estimated changes per day (e.g., how much symptom severity improved daily) along with 95% confidence intervals (CIs), which provide a range of plausible values for the true change. Additionally, interaction p-values were reported to test whether the rate of change differed significantly between groups (e.g., early vs. late therapy). A significant interaction p-value (e.g., p < 0.05) would indicate that the groups improved at different rates over time.
To complement the LME results, which focus on population-level trends, paired t-tests were used to assess within-group changes (e.g., pre- to post-therapy) for participants who completed all study timepoints. These tests compare the same individuals at two timepoints to determine if there was a significant change. For example, a paired t-test might show that symptom severity significantly decreased from pre- to post-therapy in the early therapy group. To quantify the magnitude of these changes, Hedges’ G effect sizes (ESg) were calculated. Effect sizes were interpreted as small (0.2–0.5), medium (0.5–0.8), or large (>0.8), providing context for whether the observed changes were not only statistically significant but also clinically meaningful.
In summary, despite the high dropout rates caused by the COVID-19 pandemic, as noted by the authors, the study employed robust statistical methods to minimize bias. Missing data were not extrapolated or imputed; instead, the Linear Mixed-Effects Models (LME) used all available observed data to infer population-level trends without predicting individual missing values. Sensitivity analyses confirmed the robustness of the results, demonstrating that the findings were reliable even under different assumptions. Additionally, effect sizes (Hedges’ G) were used to quantify the magnitude of the intervention’s impact on patient symptoms, providing insight into both statistical significance and clinical relevance.
Take-home messages
Early physiotherapy after traumatic brain injury leads to faster rates of improvement in key outcomes, particularly in motor activation and balance control. This study highlights valuable clinical tools—such as the SCAT5, Vestibular Ocular Motor Screening (VOMS), Mini-BESTest, and Central Sensorimotor Integration Test (CSMI)—that can be easily integrated into clinical practice for both initial assessment and test-retest purposes. These tools help ensure a comprehensive evaluation of recovery progress.
It is crucial to assess both symptom resolution and functional recovery before clearing patients to return to activities. A patient may report no symptoms but still exhibit functional limitations, putting them at risk of re-injury. This underscores the need for thorough, multidimensional assessments in mTBI management.
The findings reinforce the benefits of physiotherapy after traumatic brain injury, emphasizing the importance of advocating for the role of physical therapists within the healthcare system. By promoting early access to care and utilizing evidence- based tools, physical therapists can play a pivotal role in optimizing recovery and reducing the risk of long-term complications.
Reference
Learn to Treat the Most Common Cause of Vertigo in This FREE Mini-Video-Series
Leading Vestibular Rehabilitation Expert Firat Kesgin takes you on a 3-Day Video Course on how to recognize, assess and treat posterior canal Benign-Paroxysmal Positional Vertigo (BPPV)


