
Research
Education & Career
April 24, 2025
Improving Physiotherapy Adherence: Uncovering the Hidden Reasons Behind No-Shows & Drop-Offs

Introduction
Patient no-shows, missed appointments, and early drop-offs pose significant challenges for physiotherapy clinics—not only affecting clinic efficiency but also jeopardizing patient recovery outcomes. Patient attrition (defined as the discontinuation of care before achieving treatment goals) can lead to substantial financial losses, with some studies reporting revenue declines of up to 50.6%.
Existing research highlights several potential contributors to poor physiotherapy adherence, including patient age, socioeconomic barriers, transportation difficulties, and family-related obstacles. However, a deeper understanding of why patients disengage after their initial evaluation remains critical for improving retention strategies.
This qualitative study explores the underlying reasons patients discontinue physiotherapy early, providing actionable insights to enhance adherence and optimize care delivery.
Methods
Participants:
Participants from 18 to 89 years old, who attended an initial PT evaluation but no follow-up within 30 days were recruited from 28 clinics. Exclusions included: vestibular/non-MSK conditions, post-op cases, cognitive/communication barriers, or therapist-recommended discharge. All participants were English-proficient.
Interviews:
The interviews were recorded and transcribed, ensuring compliance with health data protection regulations. Participants provided verbal consent and could receive a written consent form afterward. The two investigators were fellowship-trained orthopedic physiotherapists with nine years of experience and formal training in qualitative research. They had no prior or ongoing clinical relationship with participants to avoid bias. The interviews were conducted privately, with only the investigator and participant present.
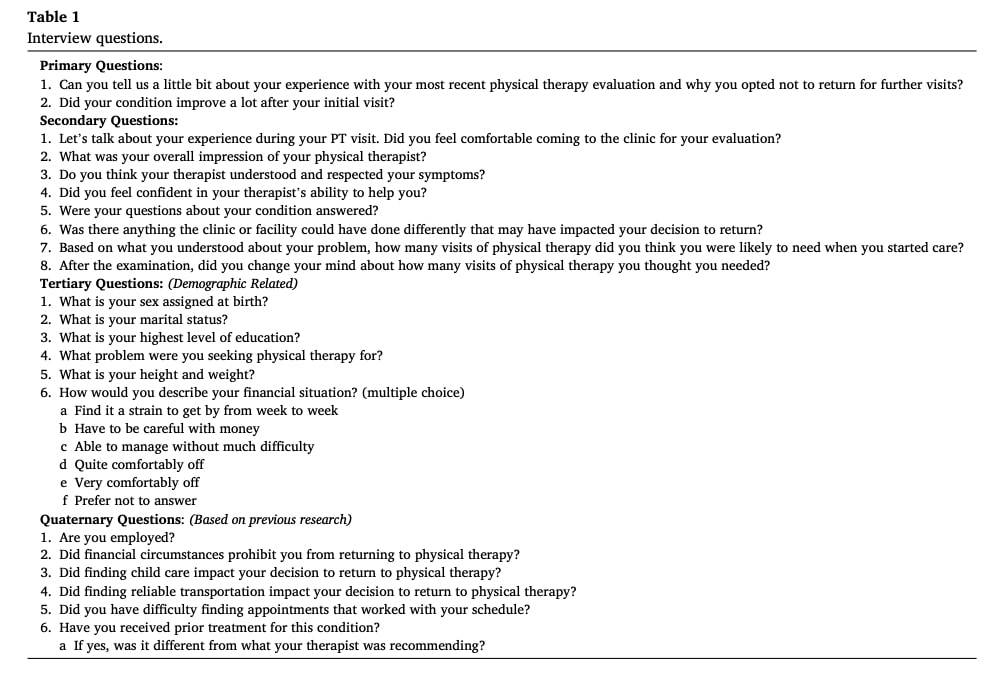
The study used a 30 minute semi-structured interviews (based on an interview guide) to explore physiotherapy adherence and why participants did not return for recommended sessions after their initial evaluation. The interviews included four sections with primary to quaternary questions, informed by existing research on missed medical appointments. Broad opening questions like “Can you tell us a little bit about your experience with your most recent physical therapy evaluation and why you opted not to return for further visits?” were followed by secondary probes such as “Was there anything the clinic or facility could have done differently that may have impacted your decision to return?” Interviews continued until no new themes emerged (stopping at 26 participants). Investigators took notes during interviews and later reviewed transcripts independently. Demographic data (e.g., age, sex, insurance) came from medical records, while additional details (e.g., social support, employment) were collected verbally during interviews.
Analysis and findings
The study employed a framework analysis approach (Nowell et al., 2017) to analyze interview data, following a six-step process: (1) familiarization with the data, (2) initial coding, (3) theme identification, (4) theme review, (5) theme definition/naming, and (6) report production. Two investigators (AT, SS) coded and indexed the transcripts using inductive reasoning, then grouped codes into primary and secondary themes via a constructivist approach. A third investigator (CC) was available to resolve coding disagreements.
Key themes and supporting quotations were organized in Microsoft Excel, while descriptive data (e.g., demographics) were analyzed in SPSS 29.0, using means for continuous variables and frequency counts for dichotomous data.
For a deeper dive into the study’s analysis methods, check out the ‘Talk Nerdy to Me’ section!
Results
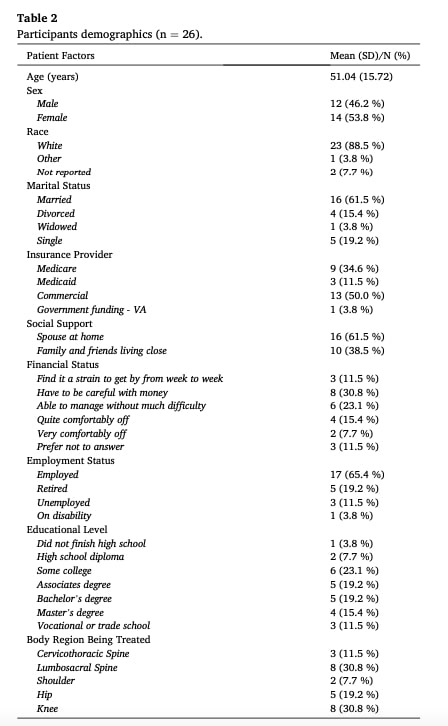
Participants characteristics: Out of 476 phone calls to potential participants, only 26 individuals (5.5% of contacted) consented and completed interviews. The 26 participants had an average age of 51 (±15.7 years), with 46% male and 88.5% White. Most were married (61.5%), employed (65.4%), and all reported having social support at home.
The study cohort (88.5% White, 46% male) closely mirrored the broader pool of 904 potential participants (91.5% White, 42.8% male), though many were excluded for falling outside the 30–90 day post-evaluation contact window.
Patient attrition themes
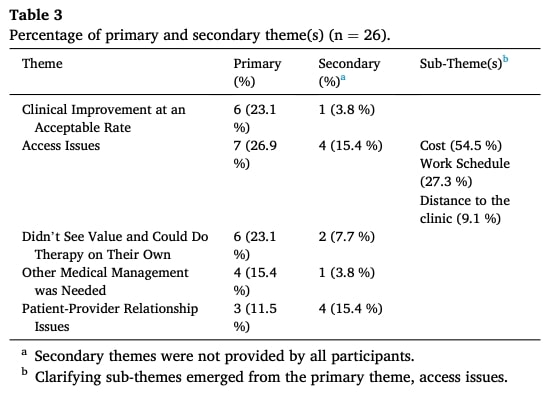
The analysis identified five key factors impacting physiotherapy adherence, revealing why participants discontinued follow-up sessions. Below are the identified themes along with supporting participant quotes
Clinical Improvement at an Acceptable Rate – Six participants cited sufficient improvement as their primary reason for discontinuing therapy, while one additional participant identified it as a secondary factor.
“The exercises they gave me helped a lot, and I improved a lot in combination with the anti-inflammatories that were prescribed to me. I didn’t feel like I had to continue with therapy.”
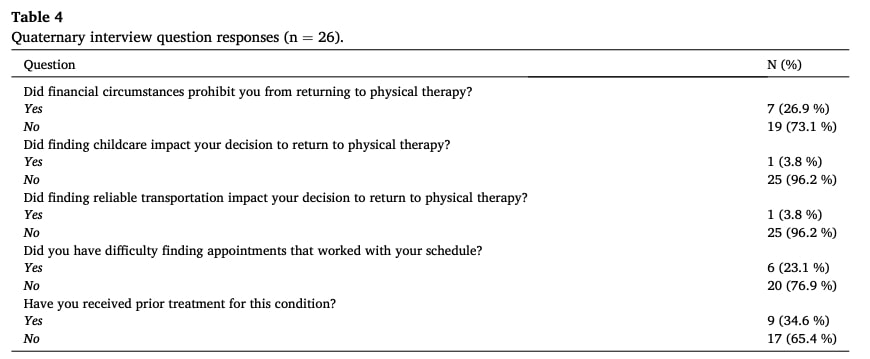
Access Issues – Seven participants identified access issues as the primary barrier to physiotherapy adherence, while four cited it as a secondary factor. The most common barrier was cost (6 participants), followed by work-clinic schedule conflicts (3). Additional obstacles included excessive travel distance (1 participant) and lack of handicap accessibility (1 participant).
“At the end of the day, you know, I have a finite amount of money.”
“I don’t have time with how my schedule was set up with work and my two kids’ schedules.”
Did Not See Value and Could Do Therapy on Their Own – Six participants believed they could continue therapy independently. Two participants reported this as a secondary reason for not returning.
“All that he [the therapist] told me to do was the same exercises which I’ve done over the last, I don’t know how many years. Nothing seems to be getting better.”
“I have to have a shoulder replacement, and it doesn’t matter how much I move my arm or whatever, it’s not gonna do no good.”
Other Medical Management Was Needed– Four participants discontinued physiotherapy because they needed to prioritize other medical treatments, while one additional participant cited this as a secondary consideration.
“It just wasn’t really helping.” This participant later went on to have a corticosteroid injection and reported “all the swelling of my calf, up in my knee, and a lot of the swelling in my ankle, like went away.”
Patient-Provider Relationship Issues – Three patients reported negative experiences or poor communication with their providers influenced their decision. Four participants indicated this was a secondary reason for not returning for subsequent visits.
“I decided not to return because I was in more pain after … I told him [the physical therapist] I did not want to be manipulated, but he was pushing … he was trying to stretch between my discs even after I said I didn’t want to be manipulated.”
“I didn’t feel like the warm and fuzzies with the practitioner or the person conducting the visit. The bedside manner just seemed cold.”
Questions and thoughts
The low response rate (5.5% of screened participants) may introduce selection bias, potentially limiting the representativeness of the findings. The study cohort may not fully capture the perspectives of non-responders, who could present distinct psychosocial characteristics influencing therapy adherence.
Additionally, the study focused on a Midwestern American population with specific socioeconomic traits, which may reduce the generalizability of results. While larger-scale studies are needed to enhance external validity, it is noteworthy that other U.S.-based studies have identified similar themes regarding barriers to adherence.
Although regional factors (e.g., rural access barriers) may locally influence dropout rates, broader strategies—such as patient-centered care—have showed to consistently improve retention across settings.
These findings underscore the need for a holistic approach to address multilevel determinants of participation, including:
- Macro-level: Healthcare system policies (e.g., cost, accessibility)
- Meso-level: Clinic-specific factors (e.g., scheduling flexibility)
- Micro-level: Individual beliefs, family dynamics, or psychological barriers
Therapists should consider these intersecting dimensions when designing interventions to optimize engagement.
Talk nerdy to me
The study used framework analysis, a structured qualitative method, to organize interview data into meaningful themes. The goal was to categorize findings into primary themes (major recurring ideas) and secondary themes (more specific sub-patterns). For example, if multiple participants mentioned cost, travel, and scheduling as barriers, those might be grouped under the primary theme “Access Issues,” with each problem as a secondary sub-theme. This hierarchical structuring helps researchers and clinicians prioritize interventions—addressing broad issues first (e.g., clinic policies) before drilling into specifics (e.g., copay reductions).
Coding is the foundational step where raw interview text is tagged with descriptive labels. Think of it like highlighting key phrases in a transcript and giving each one a shorthand name (e.g., labeling “I stopped because it was too expensive” as “Cost Barrier”). These codes are then clustered based on shared meaning to form themes. The study used inductive reasoning, meaning themes emerged organically from the data rather than being predefined. This contrasts with deductive approaches, where themes are predetermined (e.g., testing a preexisting theory that cost is the main dropout factor).
The analysis also applied a constructivist approach, which acknowledges that themes aren’t purely “discovered” but are shaped by the researchers’ interpretations and participants’ subjective experiences. For example, two analysts might code the same quote slightly differently—one emphasizing “time constraints,” another “work-life balance”—requiring discussion to align on a final theme. This approach embraces subjectivity but mitigates bias by involving multiple researchers and documenting decision-making processes (like using a third reviewer to resolve disagreements).
Finally, while the focus was qualitative, the study included basic quantitative analysis of demographic data using measures of central tendency. The mean (average) summarized continuous variables like age (51 years), while frequency counts tallied binary categories (e.g., 46% male). These stats contextualize the qualitative findings—for instance, if most participants were employed, their “scheduling conflicts” theme might differ from a retiree population. Together, these methods create a robust, multi-layered understanding of why patients drop out of PT, blending rich narrative insights with measurable trends.
Take home messages
Therapists should systematically assess potential barriers to physiotherapy adherence during the initial evaluation by acknowledging multi-level influences:
- Macro-level: Broader systemic hurdles (insurance coverage, transportation infrastructure, regional PT access).
- Meso-level: Clinic-operational factors (scheduling, telehealth options, cancellation policies).
- Micro-level: Patient-specific psychosocial dynamics (health literacy, self-efficacy, family support).
Early identification allows tailored intervention fostering physiotherapy adherence by reducing barriers.
Meso-Level (Clinic Actions)
- Flexible scheduling: Offer early/late appointments or weekend slots for working patients.
- Digital solutions: Implement online booking, automated reminders, and telehealth.
Micro-Level (Patient-Clinician Interaction)
Use patient-centered communication
- Employ active listening techniques
- Encourage respectful two-way dialogue
- Validate patient experiences
For evidence-based techniques to enhance communication and physical therapy adherence, explore our guide: Patient-Centered Communication Strategies
Provide clear patient education
- Explain their condition in understandable terms
- Discuss expectations and realistic recovery timelines
Collaborate on treatment planning
- Co-create therapeutic plans to achieve patient goals.
Master collaborative planning with Physiotutors’ guide to Shared Decision-Making in Physical Therapy
Apply motivational interviewing
- Elicit patient motivation
- Help resolve ambivalence
Want to boost patient engagement, compliance, and your physiotherapy treatment effectiveness? Check out this Physiotutors podcast on behavior change with Serena Simmons.
Reference
CHALLENGE: TAKE THE QUIZ THAT 75% OF PHYSIOTHERAPISTS FAIL
Answer these 10 short questions on essential knowledge each physiotherapist should know and find out if you score better


