
Research
Lumbar/SIJ
March 27, 2025
Cognitive Functional Therapy: Effective Relief for Pain and Disability in Chronic Low Back Pain

Introduction
Chronic low back pain (CLBP) is a major global health challenge. For most, the pain is classified as non-specific (no identifiable source) and chronic when lasting over 12 weeks. Despite its prevalence, CLBP management often falls short, with overuse of imaging, opioids, and surgery, and underuse of evidence-based, first-line treatments like the biopsychosocial model. This approach addresses the complex interplay of physical, psychological, and social factors driving pain and disability, yet many interventions still focus narrowly on the physical dimension alone.
Cognitive Functional Therapy (CFT) is a physiotherapy-led approach that integrates behavioural psychology and neuroscience to tackle the multidimensional nature of CLBP. Previous studies suggest CFT for nonspecific LBP outperforms usual care in reducing disability and is cost-effective. However, evidence remains limited. This study is the first randomized sham-controlled trial to evaluate the efficacy of CFT for pain intensity and disability in CLBP. offering a groundbreaking comparison to placebo and addressing a critical gap in the literature.
Method
To be eligible for the study, participants must be between 18 and 60 years old and diagnosed with non-specific chronic low back pain (CLBP) lasting at least 3 months, with pain localized between T12 and the gluteal folds. They must also report a pain intensity of 3 or higher on a numerical pain rating scale (NPRS) and score above 14% on the Oswestry Disability Index. Exclusion criteria include the presence of red flags (e.g., tumors, infections, fractures), serious neurological, psychiatric, rheumatologic, or cardiac conditions, specific back pathologies or a history of spinal surgery. Pregnant individuals, those who have undergone physical therapy for low back pain in the last 6 months are also excluded. Participants were instructed to avoid pain relief medications during the intervention and follow-up periods, with any medication use recorded in a pain log.
Participants were informed about the presence of a sham intervention arm and an active treatment arm. After initial assessments, participants were randomly assigned in either the CFT or sham group. Each participant was treated by a single physiotherapist, who were not involved in assessments. Participants remained blinded to their group allocation, and a blinded researcher conducted assessments at baseline, post-treatment, and follow-ups.
Primary outcomes
Pain instensity : The Numeric Pain Rating Scale (NPRS) was used to assess pain intensity. This scale ranges from 0 to 10, where 0 represents “no pain” and 10 represents “the worst pain imaginable.” The NPRS is responsive to change, with a minimum clinically important difference (MCID) of 2 for patients with chronic low back pain (CLBP).
Low back pain related disability: The Oswestry Disability Index (ODI) a questionnaire used to measure how much low back pain affects a person’s daily life. It includes 10 items covering activities like walking, sitting, and lifting, each scored from 0 to 5. The total score is converted to a percentage (0–100%), with higher scores indicating greater disability. For chronic low back pain (CLBP), the ODI has a minimum clinically important difference (MCID) of 10–12 points.
Secondary outcomes
Pain Self Efficacy Questionnaire: The Pain Self-Efficacy Questionnaire (PSEQ) includes 10 items assessing an individual’s confidence in performing tasks despite pain, rated on a 7-point scale (0: “not at all confident” to 6: “completely confident”).
Global Perceived Effect (GPE): An 11-point scale (−5: “vastly worse” to +5: “completely recovered”) asking participants to rate their back pain compared to when it first started.
Patient-Specific Functional Scale (PSFS): Patients identify up to three activities they struggle with due to their condition and rate their ability to perform each on a scale from 0 (unable) to 10 (pre-injury level).
Stanford Expectation of Treatment Scale (SETS): A 6-item scale measuring positive and negative treatment expectations, scored on a 7-point Likert scale.
Patient Health Questionnaire-9 (PHQ-9): A 9-item questionnaire screening for depression, with a cut-off score of 10 indicating possible major depression.
Generalized Anxiety Disorder-7 (GAD-7): A 7-item scale assessing anxiety severity over the past two weeks, scored from 0 to 21.
Tampa Scale for Kinesiophobia (TSK): A 17-item scale measuring fear-avoidance beliefs, scored from 17 to 68. Higher scores indicate greater fear of movement.
Pain Catastrophizing Scale (PCS): A 13-item scale assessing catastrophic thoughts about pain, scored from 0 to 52. Higher scores indicate greater pain catastrophizing.
Statistical analysis
The study included 152 patients (76 per group), designed to detect a 1-point change in pain (NPRS) and a 5-point change in disability (ODI) with 80% power, accounting for a 15% dropout rate. They used intention-to-treat analysis, meaning all participants were included, even if they didn’t finish the study. Missing data were handled with multiple imputation, and tests confirmed the missing data didn’t affect results.
Pain, disability, and other outcomes were analyzed using linear mixed models, which accounted for time (post-treatment, 3 months, 6 months) and treatment groups. When data didn’t meet normality assumptions, they used bootstrapping (a resampling method) to ensure accuracy. Effect sizes were calculated using Cohen’s d, and categorical data were analyzed with chi-square or Fisher’s exact tests.
Intervention
CFT for nonspecific LBP was delivered using a flexible, patient-centered approach, combining interviews and physical examinations to identify factors like movements, postures, pain-related beliefs, emotions, and lifestyle contributing to pain and disability. The therapist built a strong therapeutic alliance by actively listening to patients’ pain-related stories, validating their concerns, and exploring their goals. Treatment plans were tailored to individual needs and included three key components:
making sense of pain. CFT for nonspecific LBP involves a reflective process that combines the patient’s personal narrative (from interviews) and experiences to create a customized, multidimensional understanding of pain. This approach helps identify and challenge maladaptive beliefs that contribute to a vicious cycle of persistent pain and disability, encouraging healthier perspectives and behaviors.
exposure with control. The exposure with control component focuses on activities that patients report as painful, feared, or avoided, such as bending forward to pick up an object or maintaining a sitting position. Patients are guided to gradually confront these activities in a controlled manner, helping them regain confidence and reduce avoidance behaviors.
lifestyle changes. The lifestyle advice component includes guidance on gradually increasing physical activity based on patient preferences, improving sleep hygiene, managing stress, and encouraging social re-engagement. This holistic approach aims to promote long-term behavioral changes and overall well-being.
Sham intervention
Patients in the sham group received two interventions: sham photobiomodulation and neutral talking. The sham photobiomodulation will use a detuned device that emits no therapeutic dose (0J). The device will appear functional, with adjusted settings and alarms to enhance credibility. Each session will include 27 minutes of fake stimulation.
Additionally, patients were engaged in neutral talking therapy for at least 15 minutes per session. Therapists showed empathy and warmth, encouraging discussions on neutral topics like hobbies, sports, or current affairs. Maladaptive beliefs were not challenged, and any attempts to discuss emotional issues were redirected to neutral subjects. For example, if a patient says, “I guess I’ll never play soccer again because of my back pain,” the therapist might respond, “Do you like soccer? Did you watch the game on TV last week?”
After the 6-month follow-up, all participants were offered the opportunity to receive the CFT for nonspecific LBP intervention.
Results
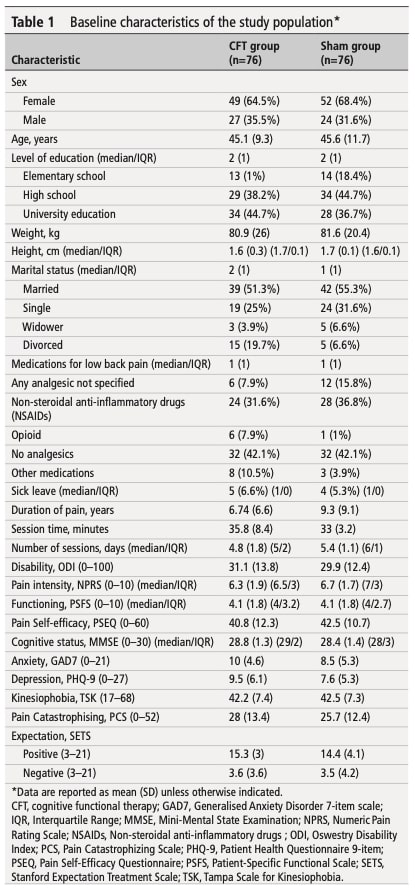
High completion rates were observed in both groups: 97-98% at post-treatment and 3-month follow-up, and 96-97% at 6-month follow-up. Baseline characteristics were similar between groups, with no significant differences (see Table 1). Both groups attended a similar mean number of sessions.
Primary outcomes
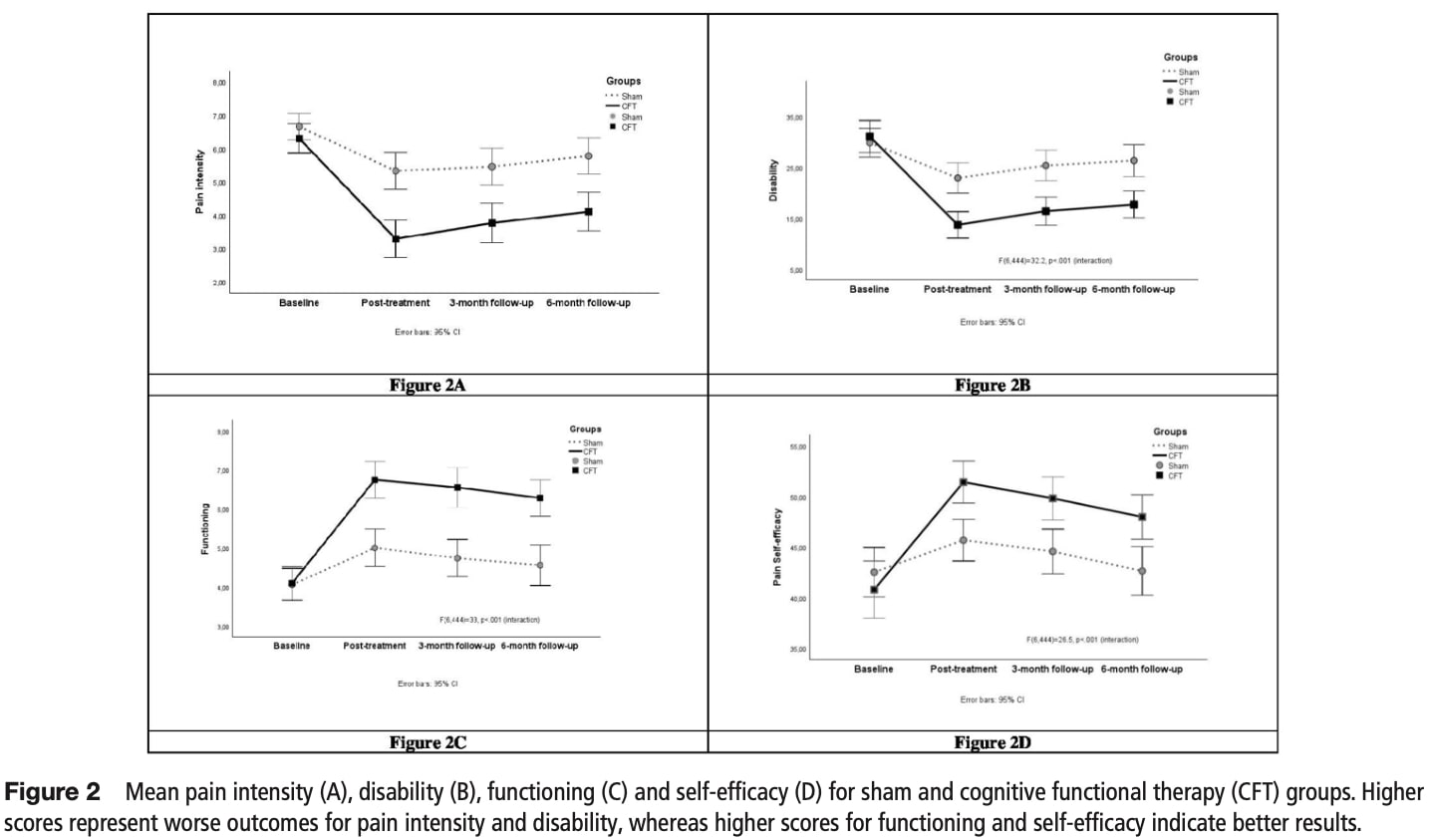
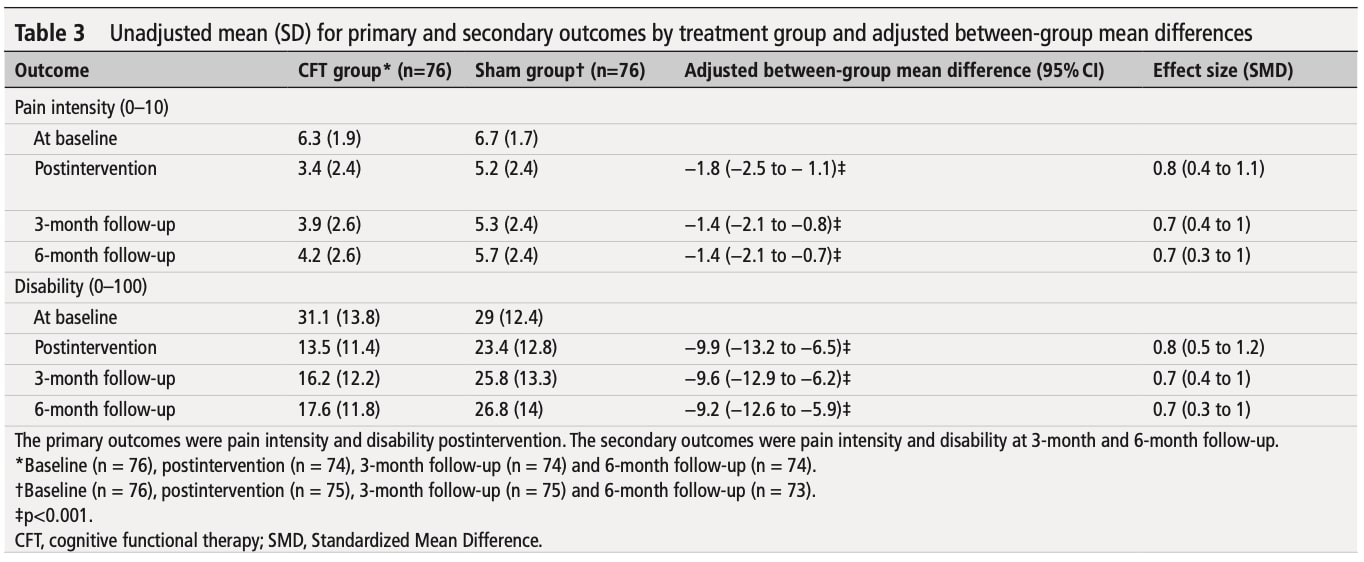
The CFT for nonspecific LBP group showed significantly greater improvements in pain intensity (mean difference = -1.8) and disability (mean difference = -9.9) compared to the sham group. Significant interactions were found between treatment, time, and baseline values for both outcomes (p < 0.001).
Secondary outcomes
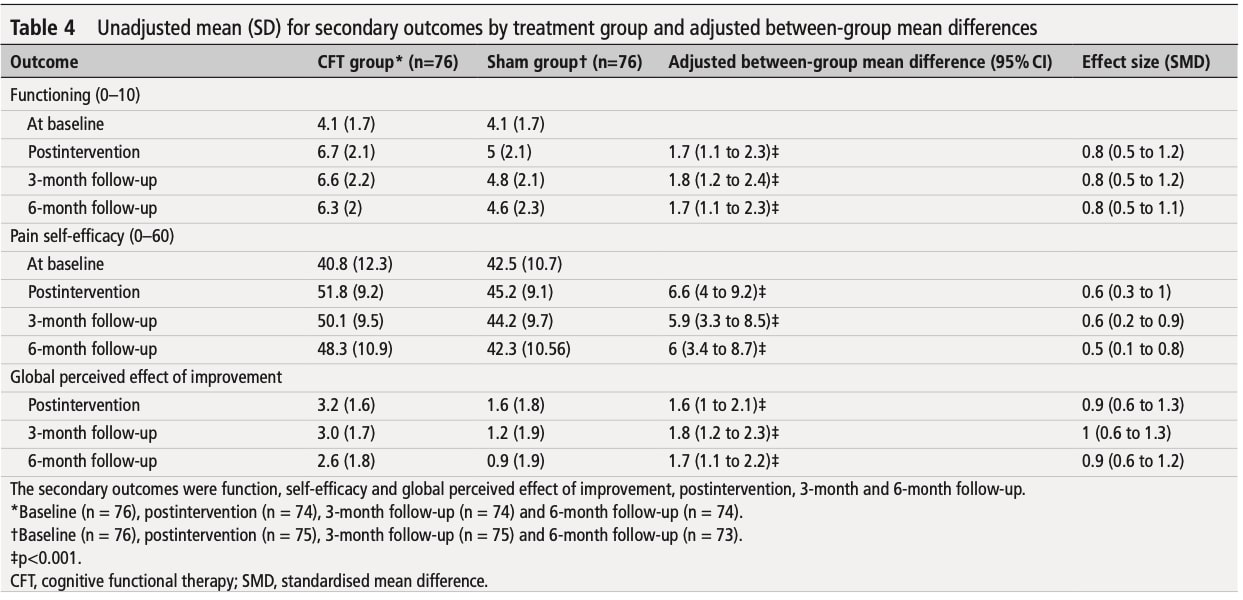
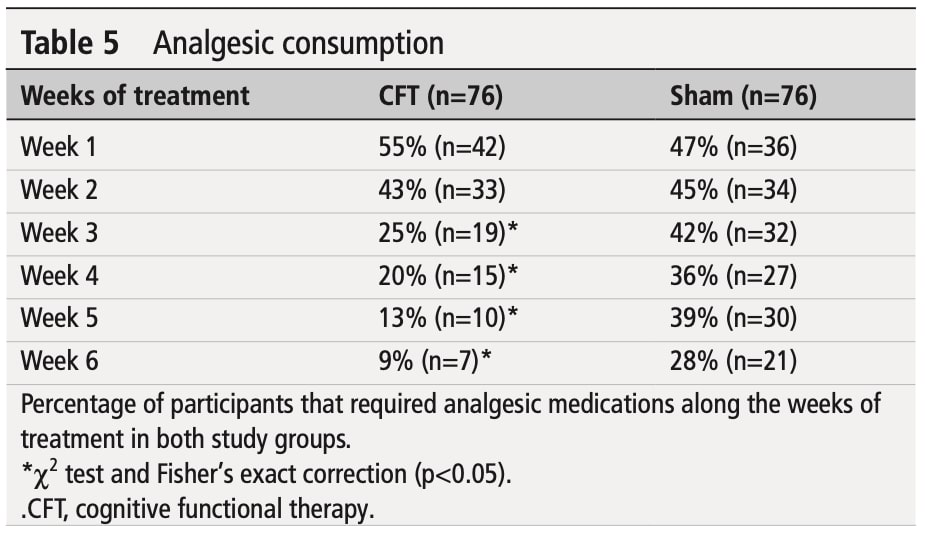
The benefits of CFT were sustained at follow-ups, with significant improvements in functioning, pain self-efficacy, and global perceived effect compared to the sham group (p < 0.001). By the third week, analgesic use decreased significantly in the CFT for nonspecific LBP group. No serious adverse events were reported.
Questions and thoughts
While validated questionnaires are useful for assessing environmental factors, they may not fully capture the complexity of pain and disability drivers. Subjective assessments and open discussions with patients can provide deeper insights into their pain experiences, helping clinicians tailor interventions more effectively.
The study did not report standard deviations (SDs), making it harder to assess variability in patient symptom evolution. Figure 2 appears to show error bars (possibly SDs), where closer lines suggest more homogeneous results. However, without clear documentation, it’s difficult to draw firm conclusions. It’s possible that patients with more complex personal and environmental drivers of pain may require multidisciplinary interventions for better outcomes.
The study found statistically significant improvements, but we must consider whether these reach the Minimal Clinically Important Difference (MCID). Using inappropriately low MCID thresholds could overestimate treatment benefits, introducing potential measurement bias. When results show significant effects below conventional MCID values, this raises important questions – are we seeing truly meaningful clinical changes, or does this suggest limitations in either the intervention or our measurement approaches?
Talk nerdy to me
The study included 152 patients (76 in each group), which was calculated to provide 80% power to detect meaningful differences—specifically, a 1-point change in pain (measured by NPRS) and a 5-point change in disability (measured by ODI). This calculation accounted for a 15% dropout rate to ensure the results would still be reliable even if some participants left the study. The researchers chose slightly smaller differences than usual (smaller than the minimally important clinical difference, MICD) to increase statistical precision, reduce the risk of Type II errors (which occur when a study fails to detect a real effect that actually exists), and ensure the groups were well-balanced.
The data were analyzed using intention-to-treat principles, meaning all participants were included in the analysis, even if they didn’t complete the study. Missing data were minimal (only 55 out of 2888 observations, or less than 2%) and assumed to be missing completely at random (MCAR). This assumption was confirmed using Little’s MCAR test, which showed no significant pattern in the missing data. In other words, the missing data were random and not linked to specific groups, time points, or outcomes. To handle these missing values, the researchers used multiple imputation, a technique that created 50 simulated datasets to estimate the missing values while preserving the relationships between key variables like treatment group, time, and outcome measures. Additionally, descriptive statistics were used to summarize the characteristics of participants in both groups, providing a clear picture of the study population.
The study used a statistical method called linear mixed models to analyze outcomes like pain, disability, and functioning over time. This method looks at how outcomes change after treatment, at 3 months, and at 6 months, while also comparing the two treatment groups (CFT vs. sham). It accounts for individual differences by treating participants as a random factor and includes baseline values to control for starting differences. Before using this method, the researchers checked if the data met certain assumptions, like whether the errors were normally distributed and whether the relationships between variables made sense. When the data didn’t meet these assumptions (except for pain), they used a technique called bootstrapping. Bootstrapping creates 1,000 simulated datasets by randomly resampling the original data, which makes the results more reliable even if the data are messy. They also used Bonferroni correction, a method that makes the significance threshold stricter (e.g., p < 0.05 becomes p < 0.01) when comparing multiple outcomes. This reduces the chance of false positives and ensures the findings are real, not just due to chance.
To measure the strength of the treatment effects, the researchers calculated effect sizes using Cohen’s d. This tells us how much difference there was between the groups in terms of pain, disability, and other outcomes. Cohen’s d uses a formula to compare the average differences between groups relative to their variability, giving a standardized result that’s easy to interpret. For analyzing categorical data (like yes/no outcomes), they used the chi-square test and Fisher’s exact test. The chi-square test checks if there’s a relationship between two categorical variables, while Fisher’s exact test is used when the sample sizes are small or when expected frequencies in the data are low (less than 5). These tests help determine if differences between groups are statistically significant.
Take home message
CFT for nonspecific LBP has shown promise in reducing pain and restoring function in patients with chronic NSLBP.
Comprehensive Assessment:
- When treating patients with chronic nonspecific low back pain (NSLBP), clinicians should evaluate pain drivers using the Pain and Disability Drivers Management Model. In this regards validated tools like the Tampa Scale for Kinesiophobia (TSK), Pain Catastrophizing Scale (PCS), Pain Self-Efficacy Questionnaire (PSEQ), and psychological health Scales (PHQ-9) (GAD-7) are insightful.
- like to identify specific patient needs and tailor rehabilitation strategies effectively.
Implementing Interventions Effectively:
- Make sense of pain: Explore the patient’s pain experience, perceptions, and dysfunctional beliefs to build a shared understanding.
- Patient Education: Educate patients about the biopsychosocial model of pain to help them understand the multifaceted nature of their condition.
- Address kinesiophobia: Use exposure to feared movements to help patients overcome fear of movement and regain confidence.
- Gradual physical activity: Encourage a gradual increase in activity levels for all patients, tailored to their pain level.
Consider Variability in Patient Responses:
- Be mindful that patients may respond differently to interventions.
- Multidisciplinary Approach: Collaborate with psychologists, physiotherapists, and other healthcare professionals to address all aspects of chronic pain.
Reference
How Nutrition Can Be a Crucial Factor for Central Sensitisation - Video Lecture
Watch this FREE video lecture on Nutrition & Central Sensitisation by Europe’s #1 chronic pain researcher Jo Nijs. Which food patients should avoid will probably surprise you!


