SLAP Lesion / Superior Labrum Tear | Diagnosis & Treatment

SLAP Lesion / Superior Labrum Tear | Diagnosis & Treatment
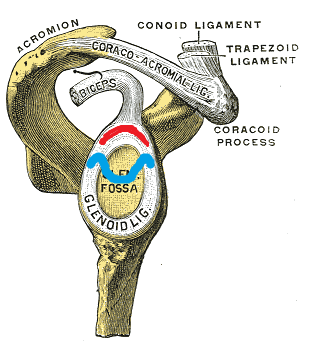
The glenoid labrum is a fibrocartilagenous structure that runs circumferentially around the rim of the shallow bony glenoid fossa, deepening the socket and acting as a passive stabilizer to prevent humeral head subluxation. The labrum also serves as an attachment site for capsuloligamentous structures, such as the glenohumeral ligaments and the long head of the biceps (Calcei et al. 2018).
SLAP stands for Superior labral tear, anterior to posterior, and comprises four major injury patterns as a cause of pain and instability, particularly in the overhead athlete (Ahsan et al. 2016).
Snyder et al. (1990) first described four injury patterns in 27 patients:
- Type I: Degenerative fraying of the superior labrum free edge with intact peripheral attachment and stable biceps tendon anchor. This pattern is very common amongst middle-aged and elderly populations, suggesting that it may be a degenerative finding that is not a definitive source of pain
- Type II: Degenerative fraying with an additional detachment of the superior labrum and biceps from the glenoid resulting in an unstable labral-biceps anchor (marked with red in the illustration)
- Type III: Bucket-handle tear of the superior labrum with an intact biceps tendon anchor (marked with blue in the illustration)
- Type IV: Lesions include a displaced bucket-handle labral tear with extension into the biceps tendon root
Ahsan et al. (2016) stress that the original description by Snyder lacks adequate reproducibility, which might partly be attributable to the difficulty in understanding even normal superior labral anatomy and age-related changes that can occur.
There are two main theories on the pathogenesis of type II SLAP lesions in athletes (Change et al. 2016):
- Cadaveric and arthroscopic demonstrations of impingement of the posterosuperior labrum between the greater tuberosity and glenoid with the shoulder in abduction and external rotation (ABER) led to the hypothesis that posterosuperior impingement causes SLAP and cuff tears.
- Other investigators favor a peel-back mechanism, wherein humeral hyper-external rotation in the late cocking phase generates a posteriorly directed torsional force on the biceps tendon, leading to twisting and peel-back and detachment of the biceps root and posterosuperior labrum from the underlying glenoid cartilage.
Given how often posterosuperior impingement, SLAP lesions, and rotator cuff undersurface tears occur concurrently, both of these proposed mechanisms likely contribute to the pathogenesis of SLAP lesions.
Acute injuries can be caused by a fall by a fall onto the outstretched arm or an unexpected pull on the arm, e.g., when losing grip of heavy objects or sudden traction (e.g., high bar exercises, hold off bodyweight in dropping rock climbers). Furthermore, injury can occur following direct contact of the adducted shoulder which an opposing player (in e.g. rugby) or to the surface (Popp et al. 2015).
Epidemiology
Schwartzberg et al. (2016) report a prevalence of up to 72% diagnosed by MRI in the asymptomatic population between 45 and 60 years of age.
Landsdown et al. (2018) retrospectively analyzed shoulder MRIs performed in patients with shoulder pain and found that the prevalence of SLAP tears increases with age. In the study, MRIs from patients between 51-65 were twice as likely to show a SLAP tear and in patients older than 65 the chance of a SLAP tear increased fourfold compared to 35-50 years of age.
On the other hand, Pappas et al. (2013) investigated the prevalence of labrum tears in 102 cadavers with an average age of 80.6 (range 57 – 96) and found a low prevalence of 9.8% with 8.8% classified as type I and 0.98% classified as type II lesions.
Weber et al. (2012) report that SLAP repairs made up 9.4% of all arthroscopic surgeries for the shoulder in the United States between 2003 and 2008 with increasing numbers.
Of those SLAP repairs, 78.4% were performed in men (mean age 36.4) and 21.6% in women (mean age 40.9).
Clinical Picture & Examination
Signs & Symptoms according to Calcei et al. (2018) are:
- Anterior shoulder pain
- Repetitive trauma through overuse
- Throwers complain about velocity and report clicking, popping during the late cocking phase of the throwing motion
- Tennis and volleyball players may complain of pain during cocking phase of the serve
- Concomitant injuries such as rotator cuff pathology and instability
Examination
Ahsan et al. (2016) state that given the difficulties in reliably classifying SLAP lesions based on arthroscopic videos, it is not surprising that physical examination maneuvers and MRI findings are reported to be unreliable in correctly diagnosing SLAP lesions.
Mathew et al. (2018) point out that a key aspect of patient history-taking is to look at the provocative phase or phases of pitching throwing in an overhead athlete.
The reason is that posterior pain in the late cocking phase could indicate a posterior superior labral tear and supraspinatus-infraspinatus junction due to internal impingement.
Posterior pain during the release or follow-through on the other hand might be indicative of the eccentric failure of the rotator cuff. Anterior pain during the cocking phase is associated with some degree of anterior instability of multifactorial origin. At last, anterior pain during the terminal phase of the throw might indicate mechanical impingement of the biceps or coracoid impingement.
Overhead throwers often present with glenohumeral internal rotation deficit (GIRD), which should be assessed first. On top of that, scapular dyskinesis is often present and should be evaluated in a second step. While we mentioned in the “Scapular Dykinesis” unit that scapular dyskinesis might actually be a sport-specific adaption, it might be a risk factor for the development of shoulder pain in athletes performing at elite levels.
Two possibly helpful clusters have been evaluated in order to exclude a SLAP lesion:
1) The “3-Pack” Examination consists of O’Brien’s Active Compression Test (ACT), resisted throwing test, and palpation of the bicipital tunnel described by Taylor et al. (2017).
The author describes that both a negative ACT (with sensitivity values ranging from 88-96% and specificity ranging from 46-64%) and/or a negative palpation test (Sensitivity: 92-98%/ Specificity: 52-73) are helpful in the exclusion of lesions to the biceps-labrum-complex.
2) The cluster described by Schlechter et al. (2009) consists of the Active Compression Test and the Passive Distraction Test (PDT). In the case of 2 positive tests, the cluster yields a LR+ of 7.0 and a negative LR- of 0.33 in the case of two negative outcomes.
Rosas et al. (2017) have conducted a literature review and have come up with a test cluster. They found that the uppercut test combined with tenderness to palpation of the long head of the biceps had the highest accuracy to diagnose pathology of the proximal biceps with a sensitivity of 88.3% and a specificity of 93.3%. Although accuracy seems to be high, this combination has not been confirmed by other studies or reviews yet, which is why we give it a moderate clinical value in practice.
TWO MYTHS BUSTED & 3 KNOWLEDGE BOMBS FOR FREE