
Research
Exercise
March 31, 2025
The Value of Prehabilitation for Total Hip Replacement

Introduction
Prehabilitation is thought to improve postoperative outcomes. Especially since muscle atrophy is often involved, bringing patients to a preoperative level of higher functional outcomes is thought to mediate postoperative recovery. Yet, systematic reviews have found conflicting results regarding the effectiveness of prehabilitation on postoperative outcomes. Hip osteoarthritis is very commonly seen, and if conservative management is insufficient, it is treated with total hip replacement. However, 7-23% of patients still experience long-term pain after the operation. Therefore, the current study looked into the effectiveness of prehabilitation for total hip replacement outcomes postoperatively.
Methods
In this two-armed randomized controlled trial, participants aged 70 years and older awaiting total hip replacement surgery were eligible candidates. They had to score 60 points or less on the Harris Hip Score, a standardized outcome measure assessing the severity of hip pain and related functional limitations.
These participants were randomly assigned to the intervention group, participating in a prehabilitation exercise intervention with patient education, or to the control group following usual care. Both the prehabilitation intervention and the control group receiving usual care completed their program before the total hip replacement surgery.
The intervention group followed this prehabilitation program for 6 to 12 weeks. Every week 3 to 4 training sessions were held, for 45 to 60 minutes each. Two of these sessions were supervised (individually or in a group), and the remaining sessions were performed at home following the instructions of the physiotherapist. The exercise program included a combination of progressive resistance training and neuromuscular training, and focused on large muscle groups. The exercises were tailored to the individual participants. Key exercises included:
- Leg press
- Leg extension
- Gluteal bridges
- Functional movements: squats, lunges, and balance exercises
The resistance exercises were performed at 40-60% of the 1RM so that 8-12 repetitions were possible, and 1 to 3 sets per exercise were performed. The exercises used bands, dumbbells, and machines. Progressions were made when tolerable but when participants rated their pain after exercise at 5 or higher on a 0-10 NRS, the dosage was lowered.
The education provided to the participants in the intervention group participating in prehabilitation included information on the management of arthritis, the importance of physical activity, and, when applicable, recommendations for weight loss. This education was provided individually or in groups.
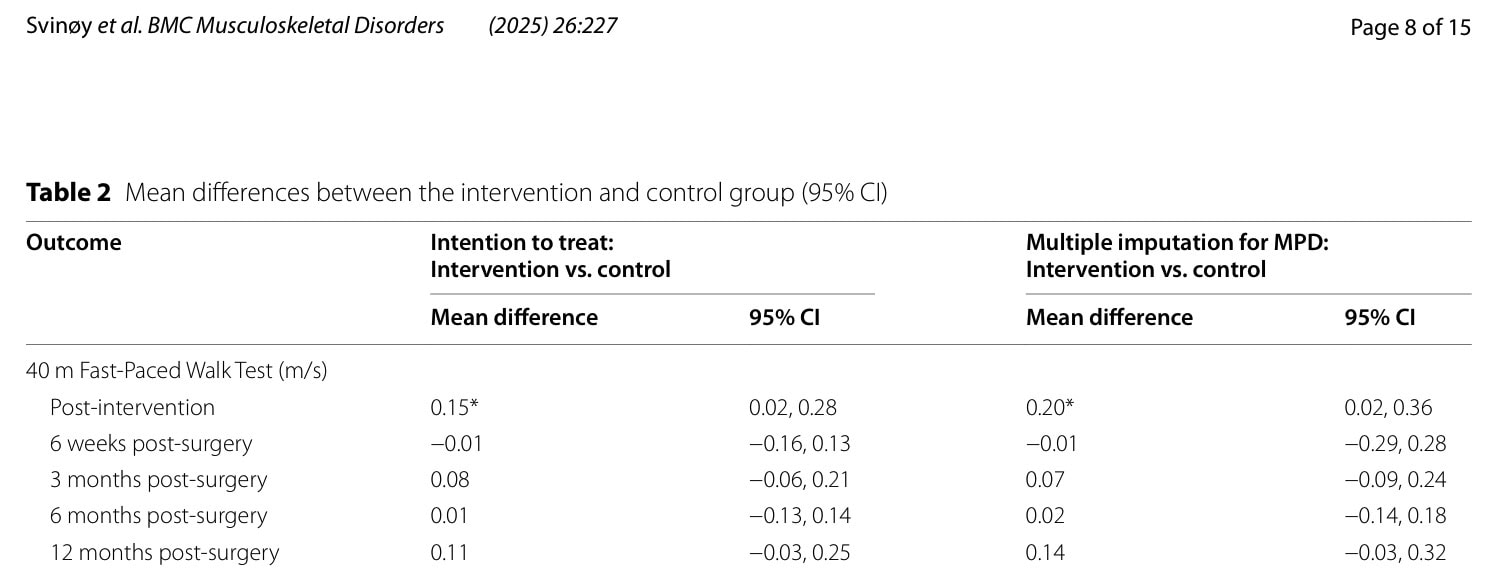
The primary outcome of interest was gait speed measured by the 40m Fast Paced Walk Test at the primary endpoint of 3 months post-surgery. Secondary outcomes included:
- Chair Stand Test
- Timed Up & Go Test
- 6 Minute Walk Test
- Stair Climb Test
- Hip Disability and Osteoarthritis Outcome Score (HOOS)
- EQ VAS for rating general health
Results
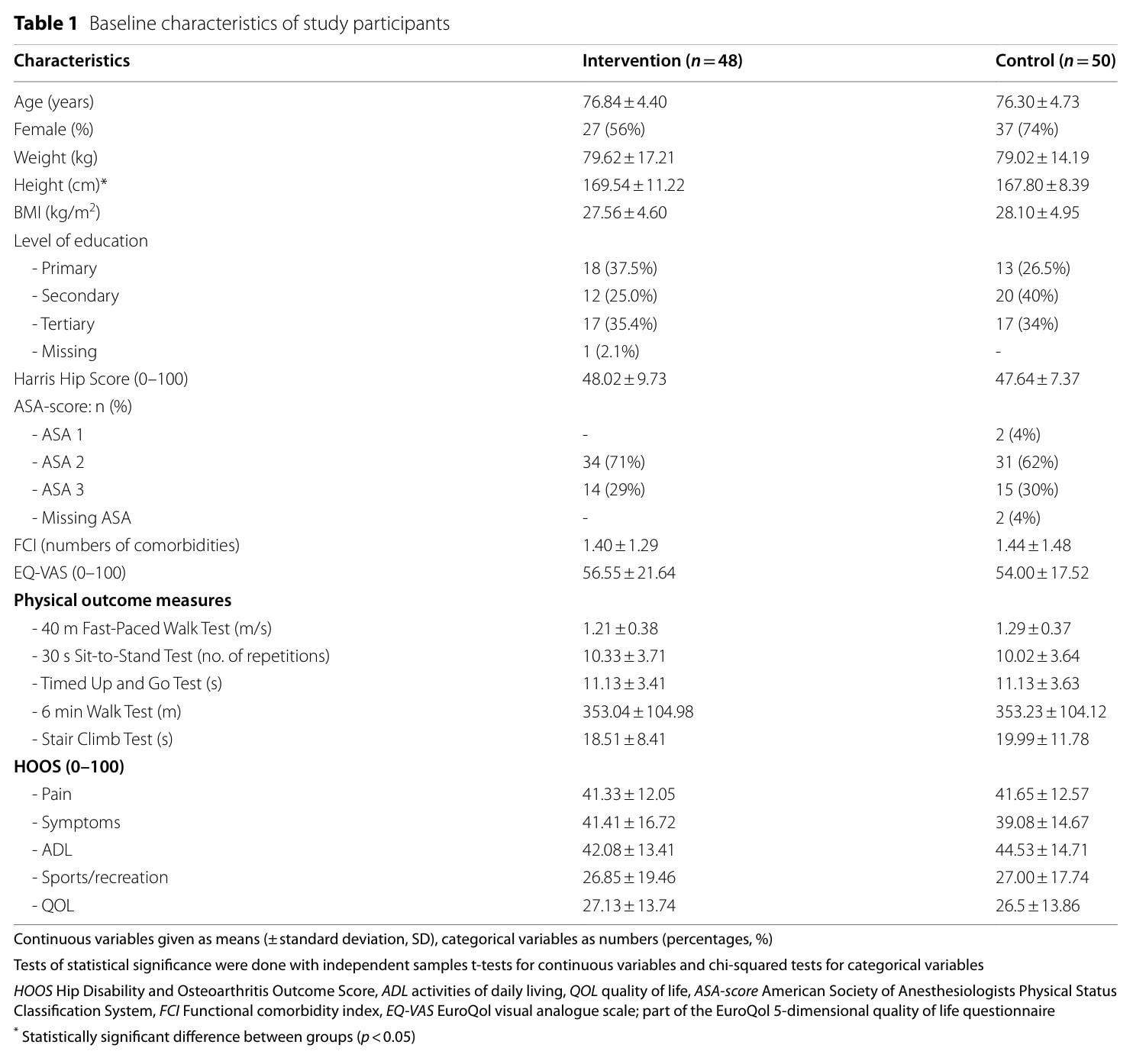
Ninety-eight individuals were recruited and randomly allocated to the intervention group (n=48) or control group (n=50). The participants were on average 76 years old and had a Harris Hip Score of 48.02 in the intervention group and 47.64 in the control group. The groups were equal at baseline, except for height, with the intervention group being approximately 2 centimeters taller.
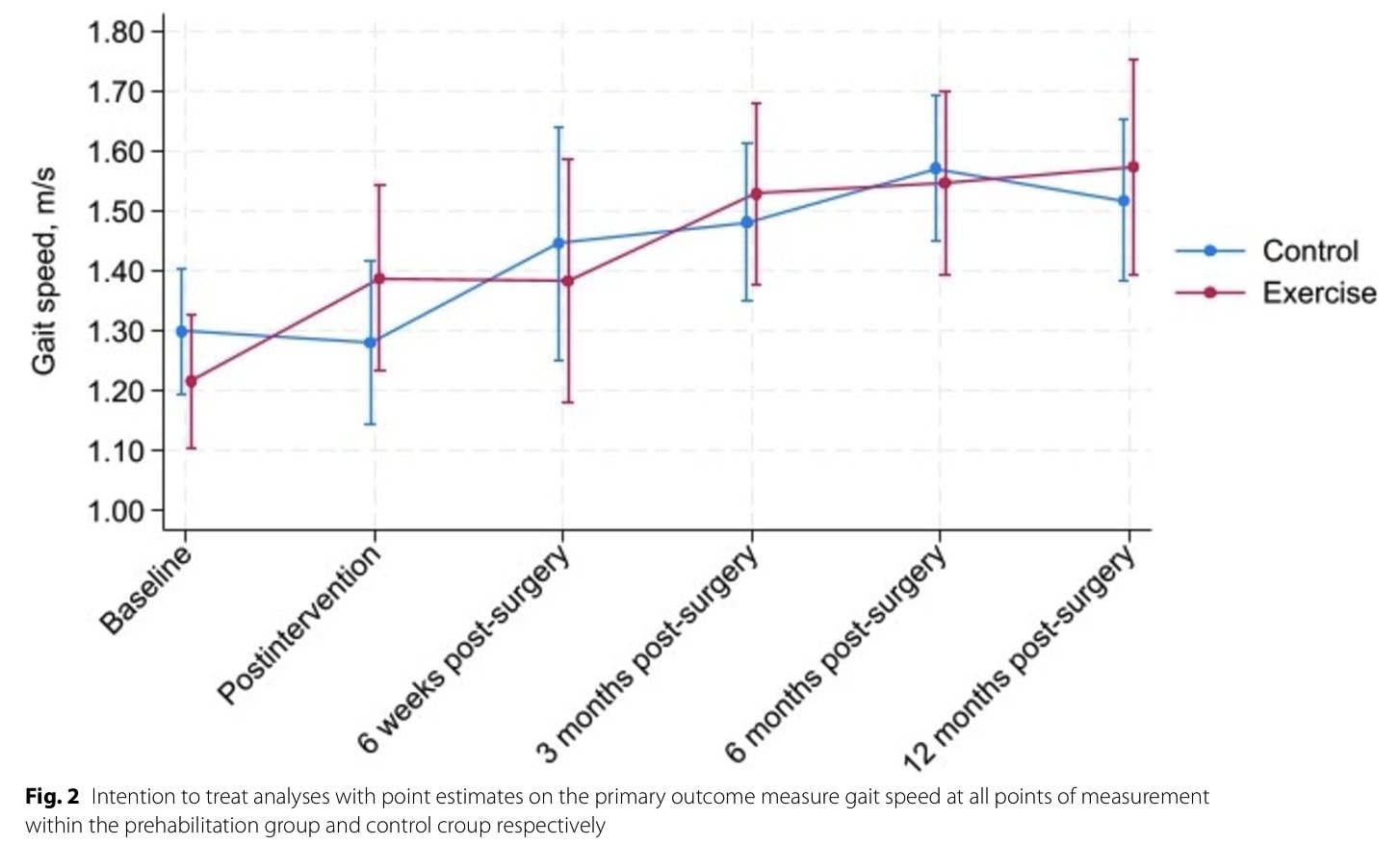
The median length of the intervention was 11 weeks, and ranged from 4-20 weeks. Two participants of the intervention group had 20 weeks of prehabilitation since their surgery was rescheduled by several weeks. At the primary endpoint, 27% of participants dropped out of the study, and no significant differences were observed between the groups regarding the primary outcome, gait speed. However, right after the intervention ended (thus before the participants underwent the surgery), a significant between-group difference favoring the prehabilitation group emerged.
None of the secondary outcome measures was statistically significant, except for the HOOS quality of life subscale post-intervention (before surgery), favoring the intervention group.
Questions and thoughts
Does prehabilitation for total hip replacement surgery offer meaningful improvements for patients with poor hip functioning awaiting surgery? Right before surgery, the prehabilitation program seems to offer a significant difference in gait speed, but this is not retained after surgery.
The authors faced large numbers of participants lost to follow-up, and the analysis of missing data showed that participants in the control group with poor baseline gait speed were more likely to drop out of the study, compared to individuals in the intervention group. This finding may have some meanings and implications. The control group participants were not informed about the importance of physical activity, and maybe they didn’t see the value of repeated physical testing after the operation. Possibly, they were feeling better after the surgical procedure and didn’t want to take part in the study anymore. Or, did they feel worse or did they got injured? If those people had worse gait speed compared to the participants who completed the study, it could mean that they were more frail and possibly susceptible to injury. Although there was no significant difference at 3 months, immediately post-intervention (before the surgery), there was a significant between-group difference in favor of prehabilitation for gait speed.
A major limitation of this study was that the treating physiotherapists indicated that it was challenging to make relevant progressions in this study population, mostly because the participants reported significant pain during and after exercise. When exercise creates pain, it may also create fear and avoidance, possibly resulting in suboptimal rehabilitation outcomes. Therefore, future research should try to make a program intensive enough, but respect individual pain responses adequately. Yet, progressive resistance training is safe and tolerable, according to Skoffer et al. 2015.
A modified version of the 6-Minute Walk test was performed, which required the participants to walk back and forth along a 15-meter straight line for 6 minutes, trying to cover as much distance as possible. This is a good alternative in the absence of treadmills, but may be more difficult for the individual, as not everyone can walk backwards fluently.
The per-protocol analysis, in which the participants who completed the trial were analyzed, showed a significant between-group difference in the 30s Chair Stand Test of 1.81 repetitions (0.01 to 3.60) more in the intervention group at 3 months and 1.89 (0.14 to 3.69) repetitions at 12 months.
Talk nerdy to me
120 participants were required in the trial, but only 98 were included at last. The authors ensured that statistical power was kept at 80%. Yet, you can not ignore the significant loss of follow-up. The majority of people were dropping out during the COVID-19 crisis. But missing data was taken into account in the analyses and the results remained consistent, so apparently this did not pose too much of a problem.
Other outcomes did not reveal significant between-group differences. There is a possibility that, since no Bonferroni correction was applied, the significance of the gait speed improvement post-intervention was a false positive finding. On the other hand, although not the primary endpoint, the missing data not at random at 6- and 12 months, potentially underestimates a possible treatment effect. The study used easy assessment methods, usable in practice, thereby enhancing its generalizability.
Take-home messages
This study concluded that prehabilitation for total hip replacement was not able to significantly alter postoperative gait speed in community-dwelling older adults at 3 months, measured by the 40-meter Fast Paced Walk test.
Reference
Learn more
LEVEL UP YOUR DIFFERENTIAL DIAGNOSIS IN RUNNING RELATED HIP PAIN - FOR FREE!
Don’t run the risk of missing out on potential red flags or ending up treating runners based on a wrong diagnosis! This webinar will prevent you to commit the same mistakes many therapists fall victim to!


