Shoulder Instability | Diagnosis & Treatment for Physiotherapists

Shoulder Instability | Diagnosis & Treatment for Physiotherapists
The shoulder joint has a tremendous degree of mobility, which renders it prone to instability. While muscle forces control stability in mid-ranges of motion, clinical instability presents itself at end range of motion (Doukas et al. 2001). It is defined as abnormal motion of the humeral head on the glenoid, which presents as pain and/or a sense of fear of displacement. Functional stability, which can be defined as maintenance of the humeral head centered within the glenoid fossa during shoulder motion, is achieved through synchronous coordination of static and dynamic components. These include negative intra-articular pressure, glenohumeral bony geometry, the capsulolabral complex, and synergistic muscle balance (Doukas et al. 2001).
The rotator cuff muscles serve to center the humeral head in the glenoid, thereby counteracting the translational forces that are generated by the prime movers of the shoulder. The glenoid labrum is known to increase the depth of the glenoid socket by approximately 50% in all directions and increases surface area as well.
Traumatic instability can range from violent forces that can frankly dislocate the joint to more subtle forces that lead to plastic deformity of the static restraints.
The mechanism of anterior dislocation is typically an abrupt abduction/external rotation force about the shoulder, while posterior most often happens due to seizures, fits, or electrocutions. It is also seen in sports with falls on the elbow, as well as tackling with an outstretched arm and a force into a posterior direction as is the case in rugby tackling.
In case of a dislocation, the following injuries are commonly seen:
- Glenoid fractures in 15 – 21% of cases (Kraeutler et al. 2018, Griffith et al. 2008)
- Bankart lesion: Detachment of the IGHL from the anterior glenoid and labrum in 84-97% of anterior dislocations (Kraeutler et al. 2018, Sedeek et al. 2014)
- Hill-Sachs lesion: Impression on the dorsal side of the humeral head after anterior dislocation in 41-83% (Kraeutler et al. 2018, Ozaki et al. 2014)
- Rotator cuff tears in 1,2% of patients in a study with a mean age of 24 (Kraeutler et al. 2018) up to 33.4% prevalence for rotator cuff tears and/or fractures of the greater tuberosity in a study with mean age of 47.6 years (Robinson et al. 2012)
- Neural injury to the axillary nerve and/or other parts of the brachial plexus in 13,5% (Robinson et al. 2012)
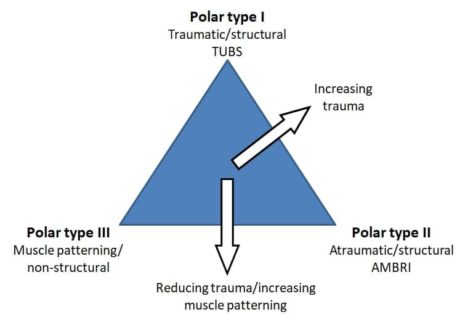 Jaggi et al. (2017) propose the Stanmore classification for the rehabilitation of shoulder instability. They mention that both structural (rotator cuff, surface area of contact, capsulolabral complex) and non-structural (central and peripheral nervous system) components are contributing to shoulder instability and stress that a continuum exists between pathologies.
Jaggi et al. (2017) propose the Stanmore classification for the rehabilitation of shoulder instability. They mention that both structural (rotator cuff, surface area of contact, capsulolabral complex) and non-structural (central and peripheral nervous system) components are contributing to shoulder instability and stress that a continuum exists between pathologies.The structural elements may be congenitally abnormal, comprise abnormal collagen, acquired micro traumatic lesions over time (atraumatic structural), or be damaged by extrinsic factors (traumatic structural). The non-structural elements can be congenitally abnormal or acquired over time as perturbations of neuromuscular control.
The Stanmore classification is as follows:
Pole I: Traumatic (TUBS = Traumatic, unilateral, Bankart lesion, surgery)
Pole II: Atraumatic (AMBRI = atraumatic, multidirectional, bilateral, rehabilitation, inferior capsular shift)
Pole III: Neuromuscular
Epidemiology
Shields et al. (2017) retrospectively examined collected trauma databases and found an incidence rate of 21.9 dislocations per 100.000 people in an urban population. They report a peak incidence of 42.1 and 50.9 in the 15-24 and ≥85 age group for males and a peak of 45.7 for females in the age group between 65 and 74.
Finhoff et al. (2004) constitute that more than 75% of cases of shoulder instability are due to trauma, with the remaining 25% categorized as non-traumatic.
Blomquist et al. (2012) report that around 75% of instabilities are in the anterior direction, most of them as a result of sports injuries or trauma.
Posterior instabilities make up around 20%, most often due to fits, seizures, or electrocutions, although sports injuries or trauma can play a role here as well.
The remaining 5% of multi-directional instability is most often seen in people with hypermobility.
Clinical Picture & Examination
It’s important to evaluate the following items in your patient history:
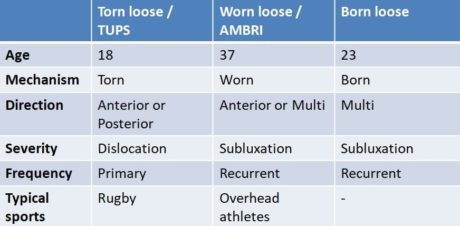
- Age: below or above 25?
- Mechanism of injury: torn (TUPS), worn (AMBRI), or born (muscle patterning / non-structural)
- The direction of instability: anterior, posterior, or multi
- Severity: dislocation or subluxation?
- Frequency: primary or recurrent
Depending on the answers, you are able to place your patient somewhere on the continuum between the 3 poles as described earlier by Jaggi et al. (2017).
It’s important to realize that psychological components like fear, anxiety and avoidance do play a role and should be evaluated as well.
Examination
After a thorough history that includes onset, circumstances, direction, frequency, and magnitude, the clinical examination is the essential first step in determining the pattern and degree of instability.
Anterior instability
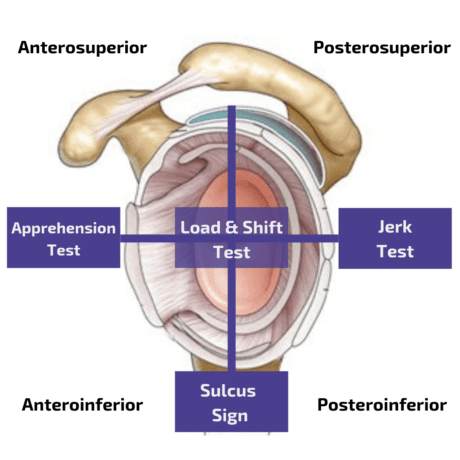
In order to evaluate anterior instability, a combination of the Apprehension and the Relocation Test yields a sensitivity of 67% with a specificity of 98%, thus basically confirming the presence of anterior structural instability (Hegedus et al. 2012).
The apprehension test is usually directly followed by the relocation test:
An additional orthopedic test that is often performed as a follow-up to the Apprehension and Relocation Test is the Release Test.
Posterior instability
Postereroinferior instability is best assessed with the Jerk Test, which is a very accurate test with a sensitivity of 90% and a specificity of 85% (Kim et al. 2004). The authors also describe that a painful Jerk Test was a predictor of failure of conservative treatment. At the same time, in the painless jerk group (with a positive test due to a clunk) 93% responded to the rehabilitation program after a mean of 4 months.
Other orthopedic tests for posterior instability are:
Inferior instability
In order to evaluate inferior instability, you can perform the Sulcus Test or Sulcus Sign. However, no sensitivity or specificity values are known for this test. At the same time, the test reached only moderate inter-rater reliability with a Kappa value of к=0.43 in a study done by Eshoj et al. (2018).
Another orthopedic test for inferior instability is the Gagey Test. In order to assess multidirectional instability, the Load and Shift Test can be performed.
In case your patient falls into the ‘Born Loose’ category, you should also assess for hypermobility. The Beighton score together with the Brighton Criteria is a method to determine if your patient is suffering from congenital hypermobility syndrome.
TWO MYTHS BUSTED & 3 KNOWLEDGE BOMBS FOR FREE